

Diagnosing, planning and evaluating osteochondral ankle defects with imaging modalities
- PMID: 26716090
- PMCID: PMC4686441
- DOI: 10.5312/wjo.v6.i11.944
Diagnosing, planning and evaluating osteochondral ankle defects with imaging modalities
Abstract
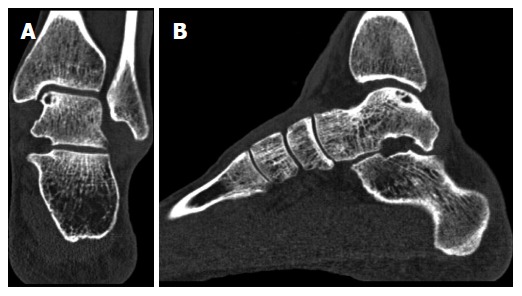
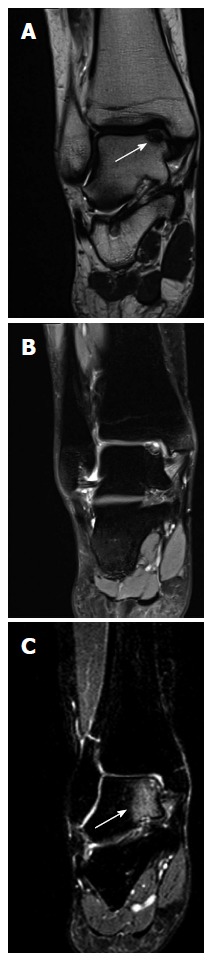
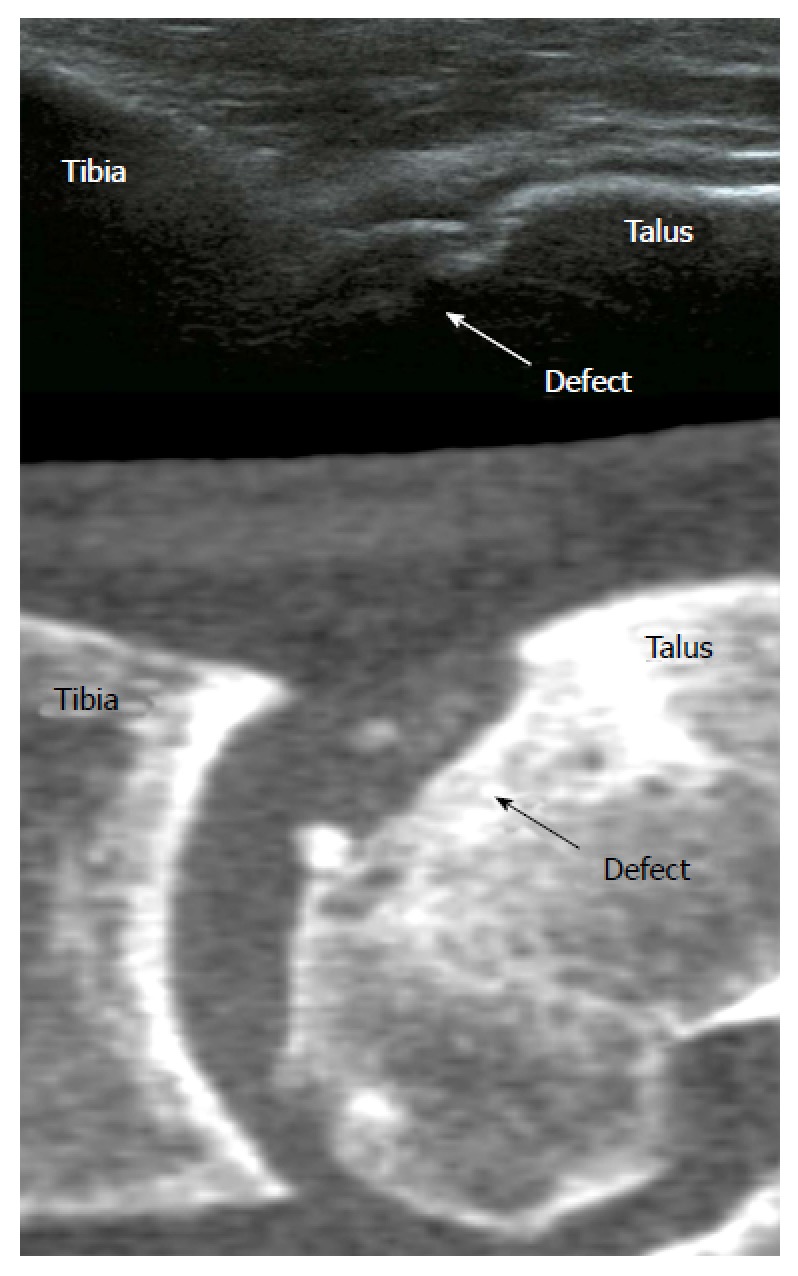
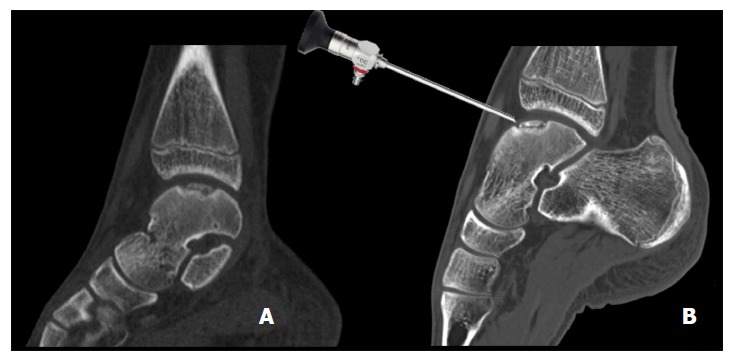
This current concepts review outlines the role of different imaging modalities in the diagnosis, preoperative planning, and follow-up of osteochondral ankle defects. An osteochondral ankle defect involves the articular cartilage and subchondral bone (usually of the talus) and is mostly caused by an ankle supination trauma. Conventional radiographs are useful as an initial imaging tool in the diagnostic process, but have only moderate sensitivity for the detection of osteochondral defects. Computed tomography (CT) and magnetic resonance imaging (MRI) are more accurate imaging modalities. Recently, ultrasonography and single photon emission CT have been described for the evaluation of osteochondral talar defects. CT is the most valuable modality for assessing the exact location and size of bony lesions. Cartilage and subchondral bone damage can be visualized using MRI, but the defect size tends to be overestimated due to bone edema. CT with the ankle in full plantar flexion has been shown a reliable tool for preoperative planning of the surgical approach. Postoperative imaging is useful for objective assessment of repair tissue or degenerative changes of the ankle joint. Plain radiography, CT and MRI have been used in outcome studies, and different scoring systems are available.
Keywords: Ankle; Cartilage; Computed tomography; Imaging; Magnetic resonance imaging; Outcome assessment; Radiography; Subchondral bone; Talus.
Figures


References
-
- Verhagen RA, Maas M, Dijkgraaf MG, Tol JL, Krips R, van Dijk CN. Prospective study on diagnostic strategies in osteochondral lesions of the talus. Is MRI superior to helical CT? J Bone Joint Surg Br. 2005;87:41–46. - PubMed
-
- Schuman L, Struijs PA, van Dijk CN. Arthroscopic treatment for osteochondral defects of the talus. Results at follow-up at 2 to 11 years. J Bone Joint Surg Br. 2002;84:364–368. - PubMed
-
- Meftah M, Katchis SD, Scharf SC, Mintz DN, Klein DA, Weiner LS. SPECT/CT in the management of osteochondral lesions of the talus. Foot Ankle Int. 2011;32:233–238. - PubMed
-
- Kok AC, Terra MP, Muller S, Askeland C, van Dijk CN, Kerkhoffs GM, Tuijthof GJ. Feasibility of ultrasound imaging of osteochondral defects in the ankle: a clinical pilot study. Ultrasound Med Biol. 2014;40:2530–2536. - PubMed
-
- van Bergen CJ, de Leeuw PA, van Dijk CN. Treatment of osteochondral defects of the talus. Rev Chir Orthop Reparatrice Appar Mot. 2008;94:398–408. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
