

Major Challenges in Clinical Management of TB/HIV Coinfected Patients in Eastern Europe Compared with Western Europe and Latin America
- PMID: 26716686
- PMCID: PMC4696866
- DOI: 10.1371/journal.pone.0145380
Major Challenges in Clinical Management of TB/HIV Coinfected Patients in Eastern Europe Compared with Western Europe and Latin America
Abstract
Objectives: Rates of TB/HIV coinfection and multi-drug resistant (MDR)-TB are increasing in Eastern Europe (EE). We aimed to study clinical characteristics, factors associated with MDR-TB and predicted activity of empiric anti-TB treatment at time of TB diagnosis among TB/HIV coinfected patients in EE, Western Europe (WE) and Latin America (LA).
Design and methods: Between January 1, 2011, and December 31, 2013, 1413 TB/HIV patients (62 clinics in 19 countries in EE, WE, Southern Europe (SE), and LA) were enrolled.
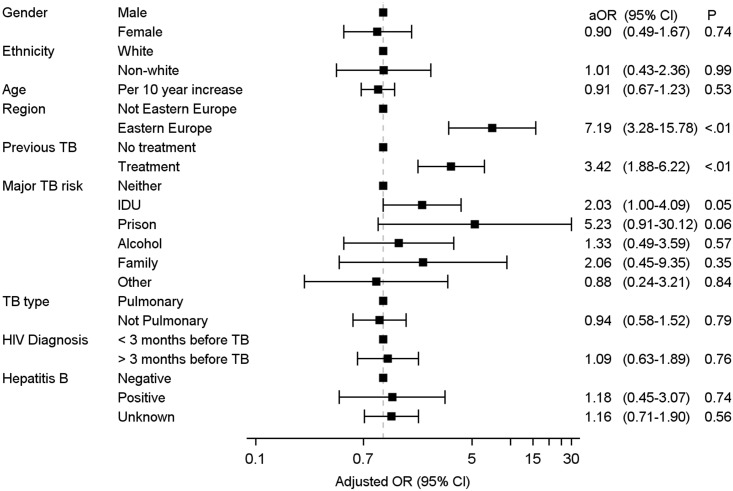
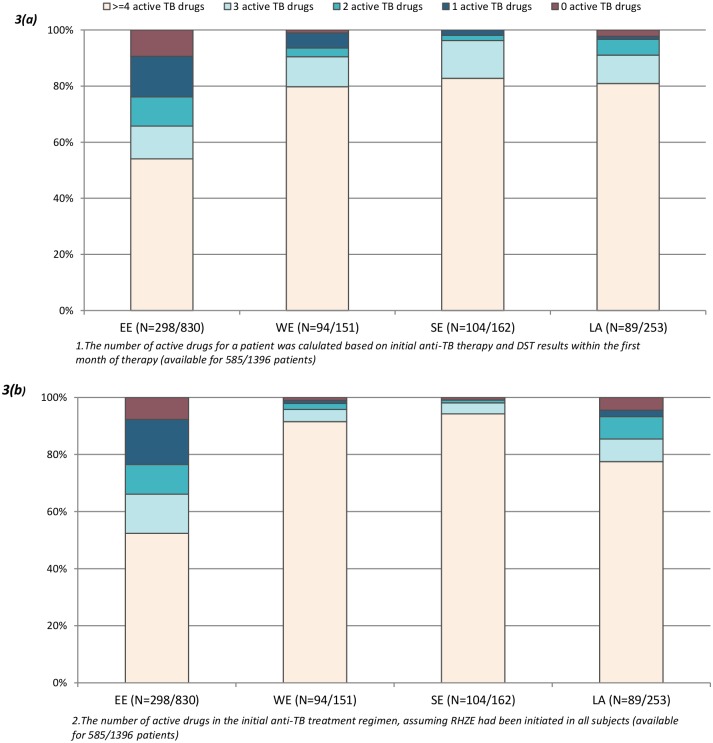
Results: Significant differences were observed between EE (N = 844), WE (N = 152), SE (N = 164), and LA (N = 253) in the proportion of patients with a definite TB diagnosis (47%, 71%, 72% and 40%, p<0.0001), MDR-TB (40%, 5%, 3% and 15%, p<0.0001), and use of combination antiretroviral therapy (cART) (17%, 40%, 44% and 35%, p<0.0001). Injecting drug use (adjusted OR (aOR) = 2.03 (95% CI 1.00-4.09), prior anti-TB treatment (3.42 (1.88-6.22)), and living in EE (7.19 (3.28-15.78)) were associated with MDR-TB. Among 585 patients with drug susceptibility test (DST) results, the empiric (i.e. without knowledge of the DST results) anti-TB treatment included ≥3 active drugs in 66% of participants in EE compared with 90-96% in other regions (p<0.0001).
Conclusions: In EE, TB/HIV patients were less likely to receive a definite TB diagnosis, more likely to house MDR-TB and commonly received empiric anti-TB treatment with reduced activity. Improved management of TB/HIV patients in EE requires better access to TB diagnostics including DSTs, empiric anti-TB therapy directed at both susceptible and MDR-TB, and more widespread use of cART.
Conflict of interest statement
Figures
References
-
- UNAIDS. UNAIDS report on the global AIDS epidemic 2013. http://wwwunaidsorg/sites/default/files/en/media/unaids/contentassets/do....
-
- Mocroft A, Lundgren JD, Sabin ML, Monforte A, Brockmeyer N, Casabona J, et al. Risk factors and outcomes for late presentation for HIV-positive persons in Europe: results from the Collaboration of Observational HIV Epidemiological Research Europe Study (COHERE). PLoS Med. 2013;10(9):e1001510 10.1371/journal.pmed.1001510 - DOI - PMC - PubMed
-
- World Health Organization. Global Tuberculosis Report 2013. http://wwwwhoint/tb/publications/global_report/en/.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
