

Planned Out-of-Hospital Birth and Birth Outcomes
- PMID: 26716916
- PMCID: PMC4791097
- DOI: 10.1056/NEJMsa1501738
Planned Out-of-Hospital Birth and Birth Outcomes
Abstract
Background: The frequency of planned out-of-hospital birth in the United States has increased in recent years. The value of studies assessing the perinatal risks of planned out-of-hospital birth versus hospital birth has been limited by cases in which transfer to a hospital is required and a birth that was initially planned as an out-of-hospital birth is misclassified as a hospital birth.
Methods: We performed a population-based, retrospective cohort study of all births that occurred in Oregon during 2012 and 2013 using data from newly revised Oregon birth certificates that allowed for the disaggregation of hospital births into the categories of planned in-hospital births and planned out-of-hospital births that took place in the hospital after a woman's intrapartum transfer to the hospital. We assessed perinatal morbidity and mortality, maternal morbidity, and obstetrical procedures according to the planned birth setting (out of hospital vs. hospital).
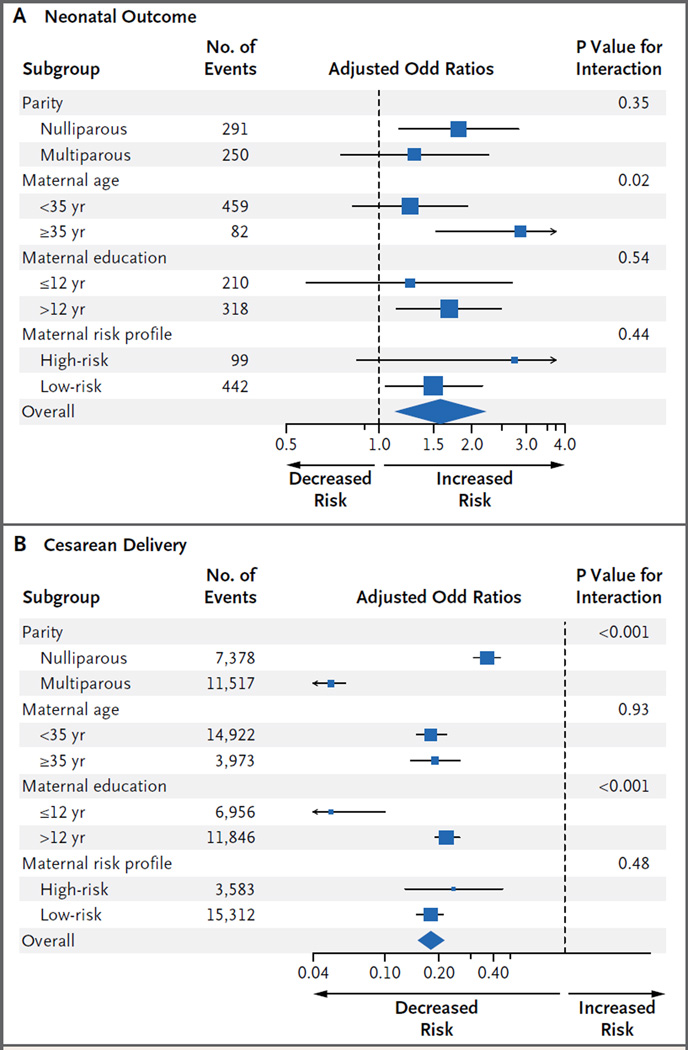
Results: Planned out-of-hospital birth was associated with a higher rate of perinatal death than was planned in-hospital birth (3.9 vs. 1.8 deaths per 1000 deliveries, P=0.003; odds ratio after adjustment for maternal characteristics and medical conditions, 2.43; 95% confidence interval [CI], 1.37 to 4.30; adjusted risk difference, 1.52 deaths per 1000 births; 95% CI, 0.51 to 2.54). The odds for neonatal seizure were higher and the odds for admission to a neonatal intensive care unit lower with planned out-of-hospital births than with planned in-hospital birth. Planned out-of-hospital birth was also strongly associated with unassisted vaginal delivery (93.8%, vs. 71.9% with planned in-hospital births; P<0.001) and with decreased odds for obstetrical procedures.
Conclusions: Perinatal mortality was higher with planned out-of-hospital birth than with planned in-hospital birth, but the absolute risk of death was low in both settings. (Funded by the Eunice Kennedy Shriver National Institute of Child Health and Human Development.).
Figures
Comment in
-
Choosing Benefits while Balancing Risks.N Engl J Med. 2015 Dec 31;373(27):2681-2. doi: 10.1056/NEJMe1511068. N Engl J Med. 2015. PMID: 26716920 No abstract available.
-
Planned Out-of-Hospital Birth and Birth Outcomes.N Engl J Med. 2016 Jun 2;374(22):2190-1. doi: 10.1056/NEJMc1602337. N Engl J Med. 2016. PMID: 27248638 No abstract available.
-
Planned Out-of-Hospital Birth and Birth Outcomes.N Engl J Med. 2016 Jun 2;374(22):2189. doi: 10.1056/NEJMc1602337. N Engl J Med. 2016. PMID: 27248639 No abstract available.
-
Planned Out-of-Hospital Birth and Birth Outcomes.N Engl J Med. 2016 Jun 2;374(22):2189-90. doi: 10.1056/NEJMc1602337. N Engl J Med. 2016. PMID: 27248640 No abstract available.
References
-
- MacDorman MF, Matthews TJ, De-clercq E. Trends in out-of-hospital births in the United States, 1990–2012. NCHS Data Brief. 2014;144:1–8. - PubMed
-
- MacDorman MF, Declercq E, Mathews TJ. Recent trends in out-of-hospital births in the United States. J Midwifery Womens Health. 2013;58:494–501. - PubMed
-
- Cheng YW, Snowden JM, King TL, Caughey AB. Selected perinatal outcomes associated with planned home births in the United States. Am J Obstet Gynecol. 2013;209(4):325.e1–328.e1. - PubMed
-
- Cheyney M, Bovbjerg M, Everson C, Gordon W, Hannibal D, Vedam S. Outcomes of care for 16,924 planned home births in the United States: the Midwives Alliance of North America Statistics Project, 2004 to 2009. J Midwifery Womens Health. 2014;59:17–27. - PubMed
-
- Stapleton SR, Osborne C, Illuzzi J. Outcomes of care in birth centers: demonstration of a durable model. J Midwifery Womens Health. 2013;58:3–14. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources