

Live-Birth Rate Associated With Repeat In Vitro Fertilization Treatment Cycles
- PMID: 26717030
- PMCID: PMC4934614
- DOI: 10.1001/jama.2015.17296
Live-Birth Rate Associated With Repeat In Vitro Fertilization Treatment Cycles
Abstract
Importance: The likelihood of achieving a live birth with repeat in vitro fertilization (IVF) is unclear, yet treatment is commonly limited to 3 or 4 embryo transfers.
Objective: To determine the live-birth rate per initiated ovarian stimulation IVF cycle and with repeated cycles.
Design, setting, and participants: Prospective study of 156,947 UK women who received 257,398 IVF ovarian stimulation cycles between 2003 and 2010 and were followed up until June 2012.
Exposures: In vitro fertilization, with a cycle defined as an episode of ovarian stimulation and all subsequent separate fresh and frozen embryo transfers.
Main outcomes and measures: Live-birth rate per IVF cycle and the cumulative live-birth rates across all cycles in all women and by age and treatment type. Optimal, prognosis-adjusted, and conservative cumulative live-birth rates were estimated, reflecting 0%, 30%, and 100%, respectively, of women who discontinued due to poor prognosis and having a live-birth rate of 0 had they continued.
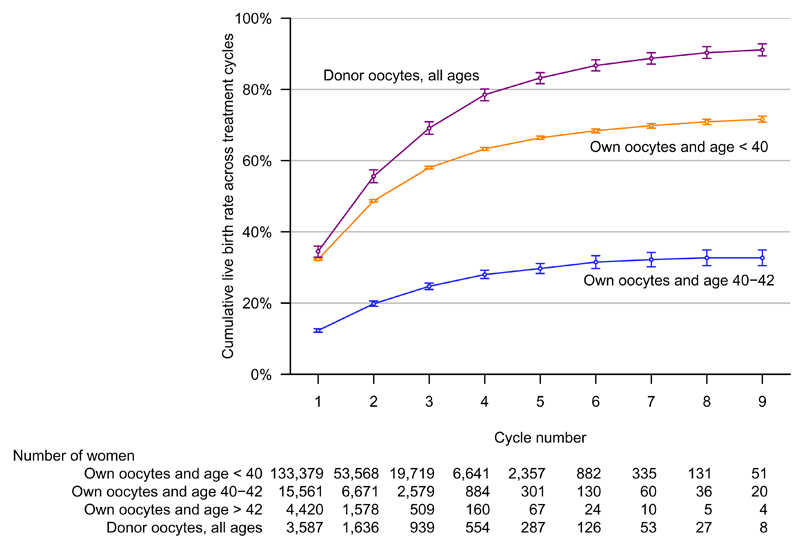
Results: Among the 156,947 women, the median age at start of treatment was 35 years (interquartile range, 32-38; range, 18-55), and the median duration of infertility for all 257,398 cycles was 4 years (interquartile range, 2-6; range, <1-29). In all women, the live-birth rate for the first cycle was 29.5% (95% CI, 29.3%-29.7%). This remained above 20% up to and including the fourth cycle. The cumulative prognosis-adjusted live-birth rate across all cycles continued to increase up to the ninth cycle, with 65.3% (95% CI, 64.8%-65.8%) of women achieving a live birth by the sixth cycle. In women younger than 40 years using their own oocytes, the live-birth rate for the first cycle was 32.3% (95% CI, 32.0%-32.5%) and remained above 20% up to and including the fourth cycle. Six cycles achieved a cumulative prognosis-adjusted live-birth rate of 68.4% (95% CI, 67.8%-68.9%). For women aged 40 to 42 years, the live-birth rate for the first cycle was 12.3% (95% CI, 11.8%-12.8%), with 6 cycles achieving a cumulative prognosis-adjusted live-birth rate of 31.5% (95% CI, 29.7%-33.3%). For women older than 42 years, all rates within each cycle were less than 4%. No age differential was observed among women using donor oocytes. Rates were lower for women with untreated male partner-related infertility compared with those with any other cause, but treatment with either intracytoplasmic sperm injection or sperm donation removed this difference.
Conclusions and relevance: Among women in the United Kingdom undergoing IVF, the cumulative prognosis-adjusted live-birth rate after 6 cycles was 65.3%, with variations by age and treatment type. These findings support the efficacy of extending the number of IVF cycles beyond 3 or 4.
Figures


Comment in
-
Extending IVF cycles beyond usual three or four shows benefit.BMJ. 2015 Dec 23;351:h6913. doi: 10.1136/bmj.h6913. BMJ. 2015. PMID: 26702087 No abstract available.
-
Repeated In Vitro Fertilization Cycles for Infertility.JAMA. 2015 Dec 22-29;314(24):2627-9. doi: 10.1001/jama.2015.17297. JAMA. 2015. PMID: 26717028 No abstract available.
References
-
- National Institute for Health and Care Excellence (NICE) Fertility: assessment and treatment for people with fertility problems. NICE clinical guideline CG156. 2013 Feb; http://guidance.nice.org.uk/CG156
-
- Berg Brigham K, Cadier B, Chevreul K. The diversity of regulation and public financing of IVF in Europe and its impact on utilization. Hum Reprod. 2013;28:666–75. - PubMed
-
- Margolioth EJ, Ben-Chetrit A, Gal M, Eldar-Geva T. Investigation and treatment of repeated implantation failure following IVF-ET. Hum Reprod. 2006;21:3036–43. - PubMed
-
- Fukuda J, Kumagai J, Kodama H, Murata M, Kawamura K, Tanaka T. Upper limit of the number of IVF-ET treatment cycles in different age groups, predicted by cumulative take-home baby rate. Acta Obstet Gynecol Scand. 2001;80:71–3. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
