

Multi-Tiered Observation and Response Charts: Prevalence and Incidence of Triggers, Modifications and Calls, to Acutely Deteriorating Adult Patients
- PMID: 26717479
- PMCID: PMC4699912
- DOI: 10.1371/journal.pone.0145339
Multi-Tiered Observation and Response Charts: Prevalence and Incidence of Triggers, Modifications and Calls, to Acutely Deteriorating Adult Patients
Abstract
Background: Observation charts are the primary tool for recording patient vital signs. They have a critical role in documenting triggers for a multi-tiered escalation response to the deteriorating patient. The objectives of this study were to ascertain the prevalence and incidence of triggers, trigger modifications and escalation response (Call) amongst general medical and surgical inpatients following the introduction of an observation and response chart (ORC).
Methods: Prospective (prevalence), over two 24-hour periods, and retrospective (incidence), over entire hospital stay, observational study of documented patient observations intended to trigger one of three escalation responses, being a MER-Medical Emergency Response [highest tier], MDT-Multidisciplinary Team [admitting team], or Nurse-senior ward nurse [lowest tier] response amongst adult general medical and surgical patients.
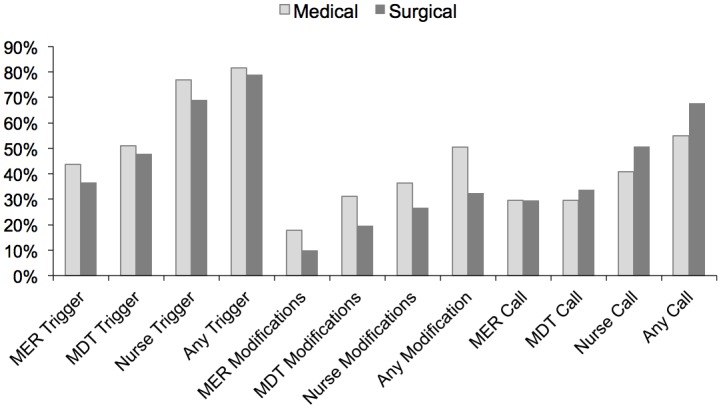
Prevalence: 416 patients, 321 (77.2%) being medical admissions, median age 76 years (IQR 62, 85) and 95 (22.8%) Not for Resuscitation (NFR). Overall, 193 (46.4%) patients had a Trigger, being 17 (4.1%) MER, 45 (10.8%) MDT and 178 (42.8%) Nurse triggers. 60 (14.4%) patients had a Call, and 72 (17.3%) a modified Trigger.
Incidence: 206 patients, of similar age, of whom 166 (80.5%) had a Trigger, 122 (59.2%) a Call, and 91 (44.2%) a modified Trigger. PREVALENCE and incidence of failure to Call was 33.2% and 68% of patients, respectively, particular for Nurse Triggers (26.7% and 62.1%, respectively). The number of Modifications, Calls, and failure to Call, correlated with the number of Triggers (0.912 [p<0.01], 0.631 [p<0.01], 0.988 [p<0.01]).
Conclusion: Within a multi-tiered response system for the detection and response to the deteriorating patient Triggers, their Modifications and failure to Call are common, particularly within the lower tiers of escalation. The number of Triggers and their Modifications may erode the structure, compliance, and potential efficacy of structured observation and response charts within a multi-tiered response system.
Conflict of interest statement
Figures

Comment in
-
Modifications to rapid response team (medical emergency team) activation criteria and its impact on patient safety.Intern Med J. 2023 Jul;53(7):1212-1217. doi: 10.1111/imj.15705. Epub 2022 May 27. Intern Med J. 2023. PMID: 35113481
References
-
- Buist M, Bernard S, Nguyen TV, Moore G, Anderson J. Association between clinical abnormal observations and subsequent in-hospital mortality: a prospective study. Resuscitation. 2004;62:137–41. - PubMed
-
- Hillman K, Bristow PJ, Chey T, Daffurn K, Jacques T, Norman SL et al. Antecedents to hospital deaths. Intern Med J 2001;31:343–8. - PubMed
-
- Trinkle R, Flabouris A. Critical Care Patient Reviews Preceding Adverse Events: Their Nature and Impact upon Patient Outcome. Resuscitation 2011;82:810–814 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
