

Preoperative radiotherapy for extremity soft tissue sarcoma; past, present and future perspectives on dose fractionation regimens and combined modality strategies
- PMID: 26718153
- PMCID: PMC5506844
- DOI: 10.1016/j.radonc.2015.12.002
Preoperative radiotherapy for extremity soft tissue sarcoma; past, present and future perspectives on dose fractionation regimens and combined modality strategies
Abstract
Introduction: This critical review aims to summarize published data on limb sparing surgery for extremity soft tissue sarcoma in combination with pre-operative radiotherapy (RT).
Methods: This review is based on peer-reviewed publications using a PubMed search on the MeSH headings "soft tissue sarcoma" AND "preoperative radiotherapy". Titles and abstracts screened for data including "fraction size AND/OR total dose AND/OR overall treatment time", "chemotherapy", "targeted agents AND/OR tyrosine kinase inhibitors", are collated. Reference lists from some articles have been studied to obtain other pertinent articles. Additional abstracts presented at international sarcoma meetings have been included as well as information on relevant clinical trials available at the ClinicalTrials.gov website.
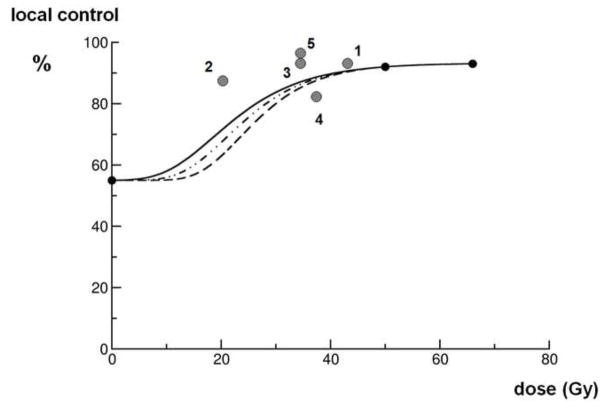
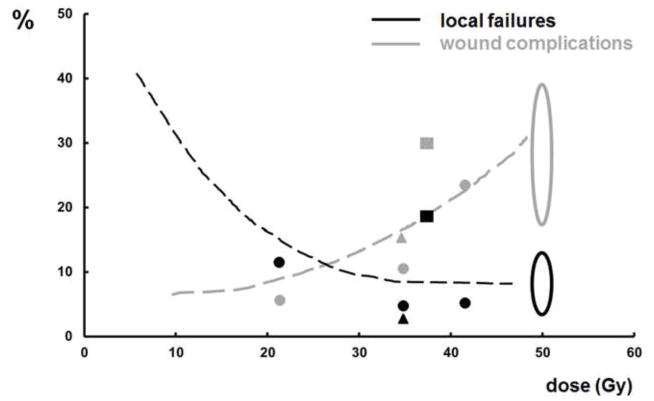
Results: Data are presented for the conventional regimen of 50-50.4Gy in 25-28 fractions in 5-6 of weeks preoperative external beam RT with respect to the regimen's local control probability compared to surgery alone, as well as acute and late toxicities. The rationale and outcome data for hypofractionated and/or reduced dose regimens are discussed. Finally, combination schedules with conventional chemotherapy and/or targeted agents are summarized.
Conclusion: Outside the setting of well-designed prospective clinical trials, the conventional 50Gy in 5-6week schedule should be considered as standard. However, current and future studies addressing alternative fraction size, total dose, overall treatment time and/or combination with chemotherapy or targeted agents may reveal regimens of equal or increased efficacy with reduced late morbidities.
Keywords: Chemotherapy; Combined modality treatment; Limb Soft Tissue Sarcoma; Preoperative radiotherapy; Surgery; Targeted agents.
Copyright © 2015 Elsevier Ireland Ltd. All rights reserved.
Conflict of interest statement
Conflicts of interest: all authors: none, except RH receiving research grants, though unrelated to the topic of this manuscript
Figures
References
-
- O’Sullivan B, Davis AM, Turcotte R, et al. Preoperative versus postoperative radiotherapy in soft tissue sarcoma of the limbs: a randomised trial. Lancet. 2002;359:2235–41. - PubMed
-
- Haas RL, Delaney TF, O’Sullivan B, et al. Radiotherapy for Management of Extremity Soft Tissue Sarcomas: Why, When, and Where? Int J Radiat Oncol Biol Phys. 2012;84:572–80. - PubMed
-
- Davis AM, Sennik S, Griffin AM, et al. Predictors of functional outcomes following limb salvage surgery for lower-extremity soft tissue sarcoma. J Surg Oncol. 2000;73:206–11. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
