

An Essential Role of NRF2 in Diabetic Wound Healing
- PMID: 26718502
- PMCID: PMC4764153
- DOI: 10.2337/db15-0564
An Essential Role of NRF2 in Diabetic Wound Healing
Abstract
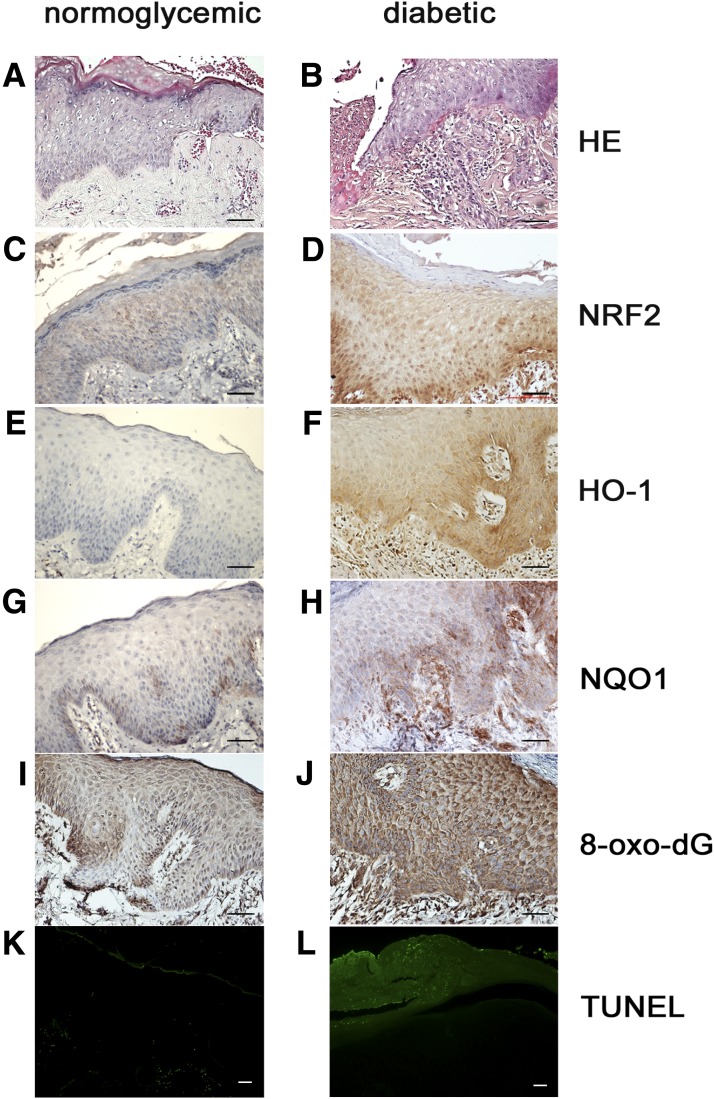
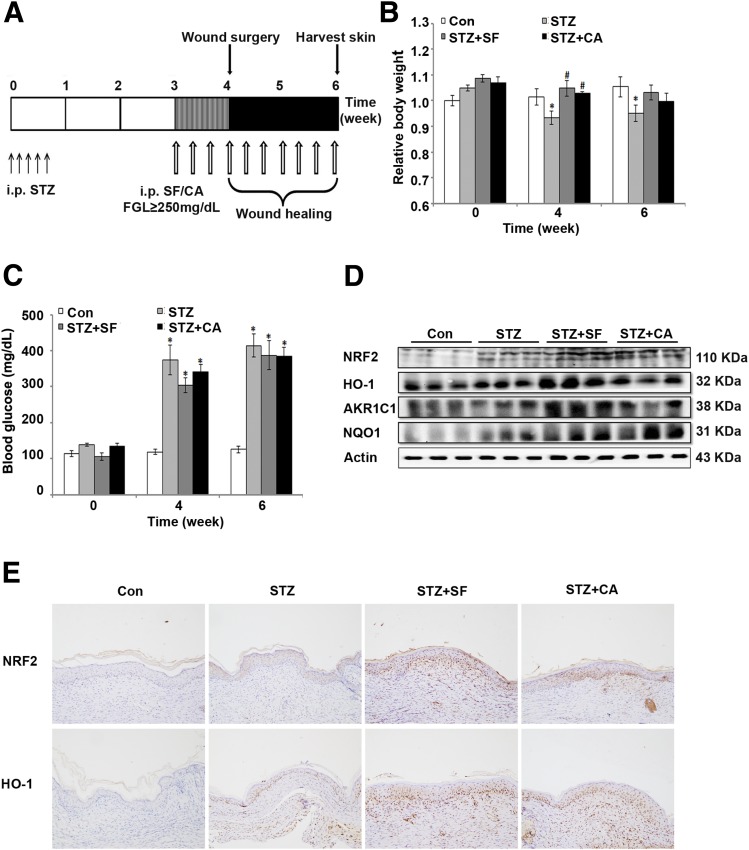
The high mortality and disability of diabetic nonhealing skin ulcers create an urgent need for the development of more efficacious strategies targeting diabetic wound healing. In the current study, using human clinical specimens, we show that perilesional skin tissues from patients with diabetes are under more severe oxidative stress and display higher activation of the nuclear factor-E2-related factor 2 (NRF2)-mediated antioxidant response than perilesional skin tissues from normoglycemic patients. In a streptozotocin-induced diabetes mouse model, Nrf2(-/-) mice have delayed wound closure rates compared with Nrf2(+/+) mice, which is, at least partially, due to greater oxidative DNA damage, low transforming growth factor-β1 (TGF-β1) and high matrix metalloproteinase 9 (MMP9) expression, and increased apoptosis. More importantly, pharmacological activation of the NRF2 pathway significantly improves diabetic wound healing. In vitro experiments in human immortalized keratinocyte cells confirm that NRF2 contributes to wound healing by alleviating oxidative stress, increasing proliferation and migration, decreasing apoptosis, and increasing the expression of TGF-β1 and lowering MMP9 under high-glucose conditions. This study indicates an essential role for NRF2 in diabetic wound healing and the therapeutic benefits of activating NRF2 in this disease, laying the foundation for future clinical trials using NRF2 activators in treating diabetic skin ulcers.
© 2016 by the American Diabetes Association. Readers may use this article as long as the work is properly cited, the use is educational and not for profit, and the work is not altered.
Figures





Comment in
-
Nrf2: a promising trove for diabetic wound healing.Ann Transl Med. 2017 Dec;5(23):469. doi: 10.21037/atm.2017.09.03. Ann Transl Med. 2017. PMID: 29285502 Free PMC article. No abstract available.
References
-
- Boulton AJ, Vileikyte L, Ragnarson-Tennvall G, Apelqvist J. The global burden of diabetic foot disease. Lancet 2005;366:1719–1724 - PubMed
-
- Falanga V. Wound healing and its impairment in the diabetic foot. Lancet 2005;366:1736–1743 - PubMed
-
- Gurtner GC, Werner S, Barrandon Y, Longaker MT. Wound repair and regeneration. Nature 2008;453:314–321 - PubMed
-
- Martin P, Parkhurst SM. Parallels between tissue repair and embryo morphogenesis. Development 2004;131:3021–3034 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
