

Overdiagnosis of idiopathic intracranial hypertension
- PMID: 26718577
- PMCID: PMC4776085
- DOI: 10.1212/WNL.0000000000002318
Overdiagnosis of idiopathic intracranial hypertension
Abstract
Objective: To delineate the factors contributing to overdiagnosis of idiopathic intracranial hypertension (IIH) among patients seen in one neuro-ophthalmology service at a tertiary center.
Methods: We retrospectively reviewed new patients referred with a working diagnosis of IIH over 8 months. The Diagnosis Error Evaluation and Research taxonomy tool was applied to cases referred with a diagnosis of IIH and a discrepant final diagnosis.
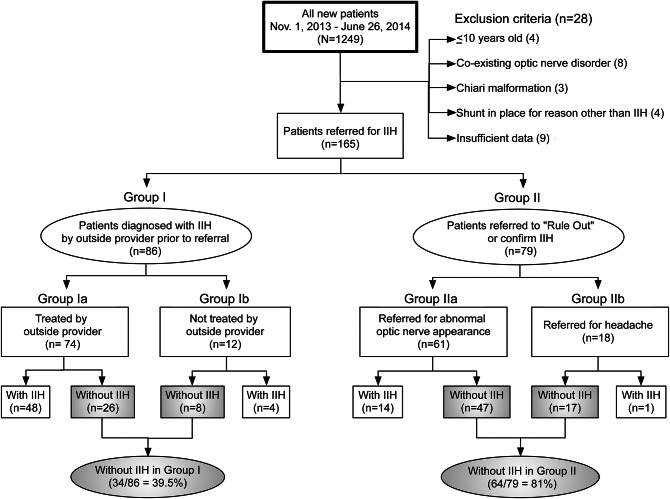
Results: Of 1,249 patients, 165 (13.2%) were referred either with a preexisting diagnosis of IIH or to rule out IIH. Of the 86/165 patients (52.1%) with a preexisting diagnosis of IIH, 34/86 (39.5%) did not have IIH. The most common diagnostic error was inaccurate ophthalmoscopic examination in headache patients. Of 34 patients misdiagnosed as having IIH, 27 (27/34 [79.4%]; 27/86 [31.4%]) had at least one lumbar puncture, 29 (29/34 [85.3%]; 29/86 [33.7%]) had a brain MRI, and 8 (8/34 [23.5%]; 8/86 [9.3%]) had a magnetic resonance/CT venogram. Twenty-six had received medical treatment, 1 had a lumbar drain, and 4 were referred for surgery. In 8 patients (8/34 [23.5%]; 8/86 [9.3%]), an alternative diagnosis requiring further evaluation was identified.
Conclusions: Diagnostic errors resulted in overdiagnosis of IIH in 39.5% of patients referred for presumed IIH, and prompted unnecessary tests, invasive procedures, and missed diagnoses. The most common errors were inaccurate ophthalmoscopic examination in headache patients and thinking biases, reinforcing the need for rapid access to specialists with experience in diagnosing optic nerve disorders. Indeed, the high prevalence of primary benign headaches and obesity in young women often leads to costly and invasive evaluations for presumed IIH.
© 2015 American Academy of Neurology.
Figures
Comment in
-
Misdiagnosing idiopathic intracranial hypertension: You've got some nerve.Neurology. 2016 Jan 26;86(4):318-9. doi: 10.1212/WNL.0000000000002320. Epub 2015 Dec 30. Neurology. 2016. PMID: 26718571 No abstract available.
-
Overdiagnosis of idiopathic intracranial hypertension.Neurology. 2016 Jun 7;86(23):2216. doi: 10.1212/WNL.0000000000002756. Neurology. 2016. PMID: 27272036 No abstract available.
References
-
- Ducros A, Biousse V. Headache arising from idiopathic changes in CSF pressure. Lancet Neurol 2015;14:655–668. - PubMed
-
- Burch RC, Loder S, Loder E, Smitherman TA. The prevalence and burden of migraine and severe headache in the United States: updated statistics from government health surveillance studies [erratum 2015;55:356]. Headache 2015;55:21–34. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources