

Incidence, Trends and Ethnic Differences of Oropharyngeal, Anal and Cervical Cancers: Singapore, 1968-2012
- PMID: 26720001
- PMCID: PMC4705110
- DOI: 10.1371/journal.pone.0146185
Incidence, Trends and Ethnic Differences of Oropharyngeal, Anal and Cervical Cancers: Singapore, 1968-2012
Abstract
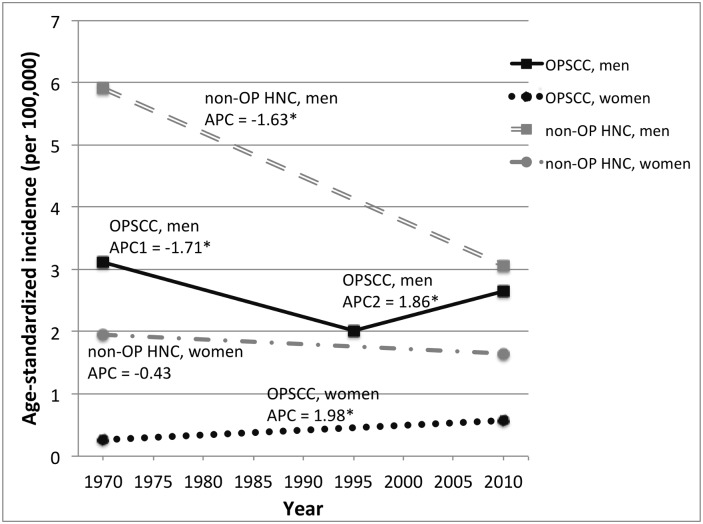
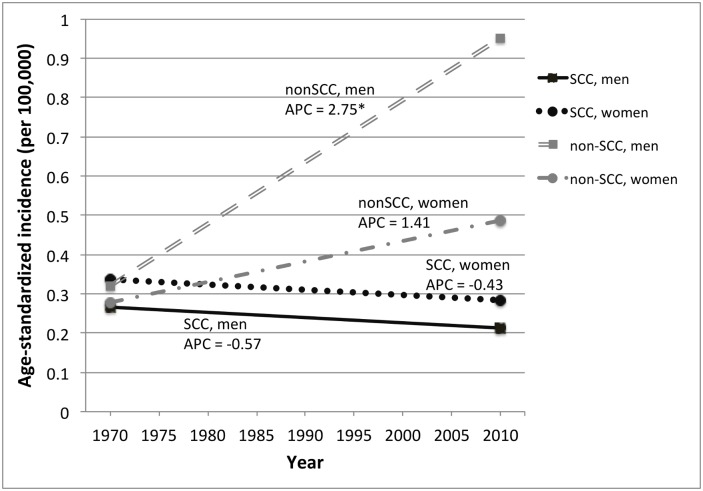
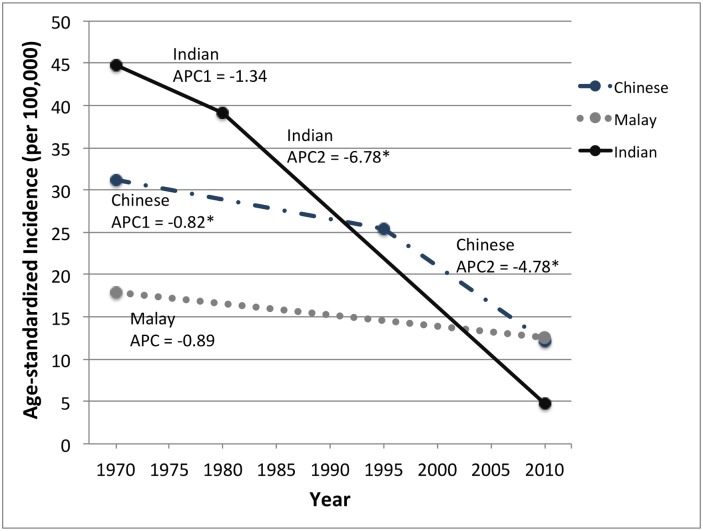
In recent decades, several Western countries have reported an increase in oropharyngeal and anal cancers caused by human papillomavirus (HPV). Trends in HPV-associated cancers in Asia have not been as well described. We describe the epidemiology of potentially HPV-related cancers reported to the Singapore Cancer Registry from 1968-2012. Analysis included 998 oropharyngeal squamous cell carcinoma (OPSCC), 183 anal squamous cell carcinoma (ASCC) and 8,019 invasive cervical cancer (ICC) cases. Additionally, 368 anal non-squamous cell carcinoma (ANSCC) and 2,018 non-oropharyngeal head and neck carcinoma (non-OP HNC) cases were included as comparators. Age-standardized incidence rates (ASR) were determined by gender and ethnicity (Chinese, Malay and Indian). Joinpoint regression was used to evaluate annual percentage change (APC) in incidence. OPSCC incidence increased in both genders (men 1993-2012, APC = 1.9%, p<0.001; women 1968-2012, APC = 2.0%, p = 0.01) and was 5 times higher in men than women. In contrast, non-OP HNC incidence declined between 1968-2012 among men (APC = -1.6%, p<0.001) and women (APC = -0.4%, p = 0.06). ASCC and ANSCC were rare (ASR = 0.2 and 0.7 per 100,000 person-years, respectively) and did not change significantly over time except for increasing ANSCCs in men (APC = 2.8%, p<0.001). ICC was the most common HPV-associated cancer (ASR = 19.9 per 100,000 person-years) but declined significantly between 1968-2012 (APC = -2.4%). Incidence of each cancer varied across ethnicities. Similar to trends in Western countries, OPSCC incidence increased in recent years, while non-OP HNC decreased. ICC remains the most common HPV-related cancer in Singapore, but Pap screening programs have led to consistently decreasing incidence.
Conflict of interest statement
Figures
Similar articles
-
Incidence trends in head and neck cancers and human papillomavirus (HPV)-associated oropharyngeal cancer in Canada, 1992-2009.Cancer Causes Control. 2012 Aug;23(8):1343-8. doi: 10.1007/s10552-012-0013-z. Epub 2012 Jun 21. Cancer Causes Control. 2012. PMID: 22718355
-
Elevated risk of human papillomavirus-related second cancers in survivors of anal canal cancer.Cancer. 2017 Oct 15;123(20):4013-4021. doi: 10.1002/cncr.30828. Epub 2017 Jun 13. Cancer. 2017. PMID: 28608917
-
Racial and ethnic differences in HPV-related cancer incidence in the United States, 2001-2020.J Natl Cancer Inst. 2025 Aug 1;117(8):1655-1663. doi: 10.1093/jnci/djaf107. J Natl Cancer Inst. 2025. PMID: 40289254
-
Human papillomavirus in cervical cancer and oropharyngeal cancer: One cause, two diseases.Cancer. 2017 Jun 15;123(12):2219-2229. doi: 10.1002/cncr.30588. Epub 2017 Mar 27. Cancer. 2017. PMID: 28346680 Review.
-
The Human Papillomavirus as a Common Pathogen in Oropharyngeal, Anal and Cervical Cancers.Clin Oncol (R Coll Radiol). 2019 Feb;31(2):81-90. doi: 10.1016/j.clon.2018.10.004. Epub 2018 Oct 29. Clin Oncol (R Coll Radiol). 2019. PMID: 30385006 Review.
Cited by
-
Social determinants of sex disparities in cancer in Southeast Asia.iScience. 2023 Jun 14;26(7):107110. doi: 10.1016/j.isci.2023.107110. eCollection 2023 Jul 21. iScience. 2023. PMID: 37456827 Free PMC article. Review.
-
Intracuff local anesthetic to reduce postoperative sore throat: a randomized clinical trial.Can J Anaesth. 2020 Apr;67(4):495-497. doi: 10.1007/s12630-019-01517-2. Epub 2019 Nov 4. Can J Anaesth. 2020. PMID: 31686363 Clinical Trial. No abstract available.
-
Malignant ureteral obstruction: comparison of metallic, 8 French and 6 French ureteric stents after failure of initial ureteric stent.World J Urol. 2024 Feb 22;42(1):92. doi: 10.1007/s00345-024-04803-x. World J Urol. 2024. PMID: 38386090
-
Investigating epidemiologic trends and the geographic distribution of patients with anal squamous cell carcinoma throughout Canada.Curr Oncol. 2020 Jun;27(3):e294-e306. doi: 10.3747/co.27.6061. Epub 2020 Jun 1. Curr Oncol. 2020. PMID: 32669936 Free PMC article.
-
Negative terpinen-4-ol modulate potentially malignant and malignant lingual lesions induced by 4-nitroquinoline-1-oxide in rat model.Naunyn Schmiedebergs Arch Pharmacol. 2022 Nov;395(11):1387-1403. doi: 10.1007/s00210-022-02275-7. Epub 2022 Aug 9. Naunyn Schmiedebergs Arch Pharmacol. 2022. PMID: 35943514
References
-
- Kreimer AR, Bhatia RK, Messeguer AL, Gonzalez P, Herrero R, Giuliano AR. Oral human papillomavirus in healthy individuals: a systematic review of the literature. Sexually transmitted diseases. 2010;37(6):386–91. . - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
