

Adherence to an Accelerated Diagnostic Protocol for Chest Pain: Secondary Analysis of the HEART Pathway Randomized Trial
- PMID: 26720295
- PMCID: PMC4716613
- DOI: 10.1111/acem.12835
Adherence to an Accelerated Diagnostic Protocol for Chest Pain: Secondary Analysis of the HEART Pathway Randomized Trial
Abstract
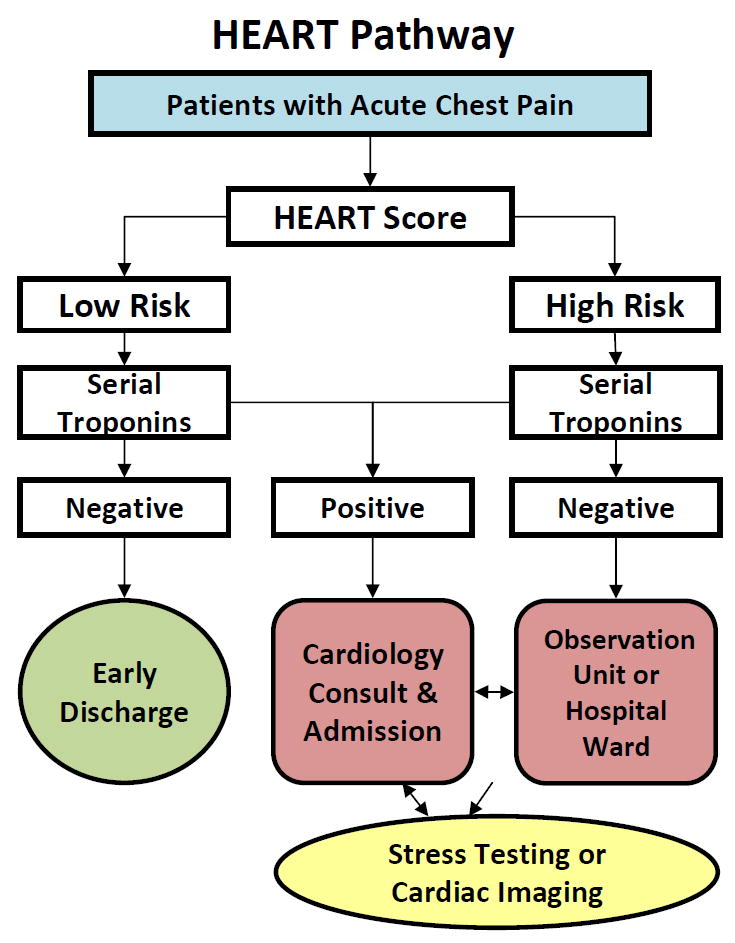
Objectives: Accelerated diagnostic protocols (ADPs), such as the HEART Pathway, are gaining popularity in emergency departments (EDs) as tools used to risk stratify patients with acute chest pain. However, provider nonadherence may threaten the safety and effectiveness of ADPs. The objective of this study was to determine the frequency and impact of ADP nonadherence.
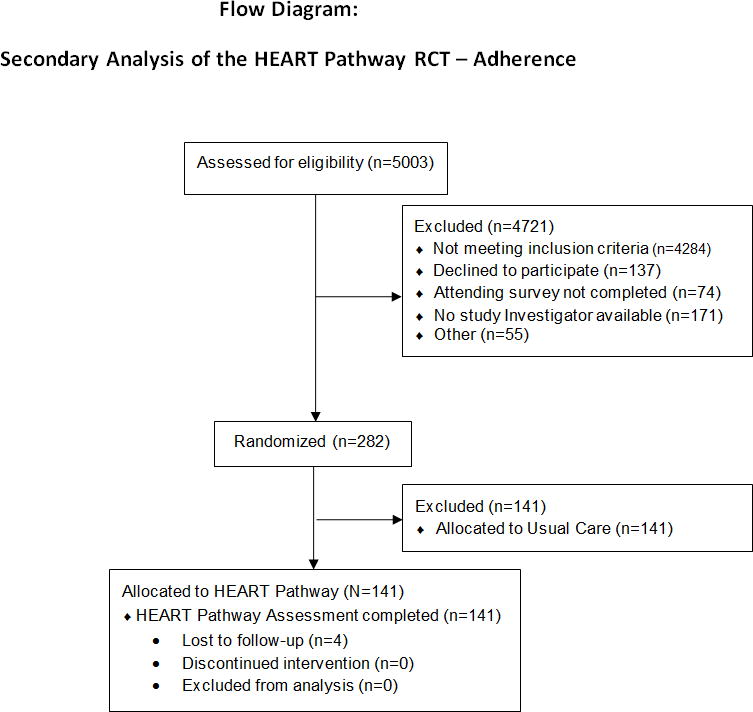
Methods: A secondary analysis of participants enrolled in the HEART Pathway RCT was conducted. This trial enrolled 282 adult ED patients with symptoms concerning for acute coronary syndrome without ST-elevation on electrocardiogram. Patients randomized to the HEART Pathway (N = 141) were included in this analysis. Outcomes included index visit disposition, nonadherence, and major adverse cardiac events (MACEs) at 30 days. MACE was defined as death, myocardial infarction, or revascularization. Nonadherence was defined as: 1) undertesting-discharging a high-risk patient from the ED without objective testing (stress testing or coronary angiography) or 2) overtesting-admitting or obtaining objective testing on a low-risk patient.
Results: Nonadherence to the HEART Pathway occurred in 28 of 141 patients (20%, 95% confidence interval [CI] = 14% to 27%). Overtesting occurred in 19 of 141 patients (13.5%, 95% CI = 8% to 19%) and undertesting in nine of 141 patients (6%, 95% CI = 3% to 12%). None of these 28 patients suffered MACE. The net effect of nonadherence was 10 additional admissions among patients identified as low-risk and appropriate for early discharge (absolute decrease in discharge rate of 7%, 95% CI = 3% to 13%).
Conclusions: Real-time use of the HEART Pathway resulted in a nonadherence rate of 20%, mostly due to overtesting. None of these patients had MACE within 30 days. Nonadherence decreased the discharge rate, attenuating the HEART Pathway's impact on health care use.
© 2015 by the Society for Academic Emergency Medicine.
Figures
References
-
- Owens PL, Barrett ML, Gibson TB, Andrews RM, Weinick RM, Mutter RL. Emergency department care in the United States: a profile of national data sources. Ann Emerg Med. 2010;56:150–65. - PubMed
-
- Litt HI, Gatsonis C, Snyder B, et al. CT angiography for safe discharge of patients with possible acute coronary syndromes. N Engl J Med. 2012;366:1393–403. - PubMed
-
- Heller GV, Stowers SA, Hendel RC, et al. Clinical value of acute rest technetium-99m tetrofosmin tomographic myocardial perfusion imaging in patients with acute chest pain and nondiagnostic electrocardiograms. J Am Coll Cardiol. 1998;31:1011–7. - PubMed
-
- Roberts R, Kleiman NS. Earlier diagnosis and treatment of acute myocardial infarction necessitates the need for a ’new diagnostic mind-set’. Circulation. 1994;89:872–81. - PubMed
-
- Hoffmann U, Nagurney JT, Moselewski F, et al. Coronary multidetector computed tomography in the assessment of patients with acute chest pain. Circulation. 2006;114:2251–60. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
