

Goal-directed Hemostatic Resuscitation of Trauma-induced Coagulopathy: A Pragmatic Randomized Clinical Trial Comparing a Viscoelastic Assay to Conventional Coagulation Assays
- PMID: 26720428
- PMCID: PMC5432433
- DOI: 10.1097/SLA.0000000000001608
Goal-directed Hemostatic Resuscitation of Trauma-induced Coagulopathy: A Pragmatic Randomized Clinical Trial Comparing a Viscoelastic Assay to Conventional Coagulation Assays
Abstract
Background: Massive transfusion protocols (MTPs) have become standard of care in the management of bleeding injured patients, yet strategies to guide them vary widely. We conducted a pragmatic, randomized clinical trial (RCT) to test the hypothesis that an MTP goal directed by the viscoelastic assay thrombelastography (TEG) improves survival compared with an MTP guided by conventional coagulation assays (CCA).
Methods: This RCT enrolled injured patients from an academic level-1 trauma center meeting criteria for MTP activation. Upon MTP activation, patients were randomized to be managed either by an MTP goal directed by TEG or by CCA (ie, international normalized ratio, fibrinogen, platelet count). Primary outcome was 28-day survival.
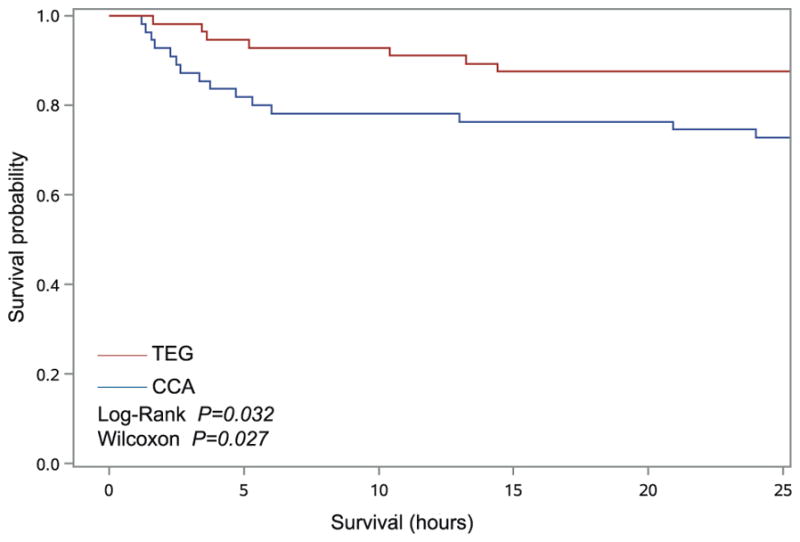
Results: One hundred eleven patients were included in an intent-to-treat analysis (TEG = 56, CCA = 55). Survival in the TEG group was significantly higher than the CCA group (log-rank P = 0.032, Wilcoxon P = 0.027); 20 deaths in the CCA group (36.4%) compared with 11 in the TEG group (19.6%) (P = 0.049). Most deaths occurred within the first 6 hours from arrival (21.8% CCA group vs 7.1% TEG group) (P = 0.032). CCA patients required similar number of red blood cell units as the TEG patients [CCA: 5.0 (2-11), TEG: 4.5 (2-8)] (P = 0.317), but more plasma units [CCA: 2.0 (0-4), TEG: 0.0 (0-3)] (P = 0.022), and more platelets units [CCA: 0.0 (0-1), TEG: 0.0 (0-0)] (P = 0.041) in the first 2 hours of resuscitation.
Conclusions: Utilization of a goal-directed, TEG-guided MTP to resuscitate severely injured patients improves survival compared with an MTP guided by CCA and utilizes less plasma and platelet transfusions during the early phase of resuscitation.
Conflict of interest statement
The author reports no conflicts of interest.
Figures


Comment in
-
To TEG, or Not to TEG: That Is the Question.Ann Surg. 2016 Jun;263(6):1060-1. doi: 10.1097/SLA.0000000000001756. Ann Surg. 2016. PMID: 27172100 No abstract available.
References
-
- Rhee P, Joseph B, Pandit V, et al. Increasing trauma deaths in the United States. Ann Surg. 2014;260:13–21. - PubMed
-
- Norton R, Kobusingye O. Injuries. N Engl J Med. 2013;368:1723–1730. - PubMed
-
- MacKenzie EJ, Rivara FP, Jurkovich GJ, et al. A national evaluation of the effect of trauma-center care on mortality. N Engl J Med. 2006;354:366–378. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
