

Paraneoplastic pemphigus associated with follicular dendritic cell sarcoma: report of a case and review of literature
- PMID: 26722384
- PMCID: PMC4680329
Paraneoplastic pemphigus associated with follicular dendritic cell sarcoma: report of a case and review of literature
Abstract
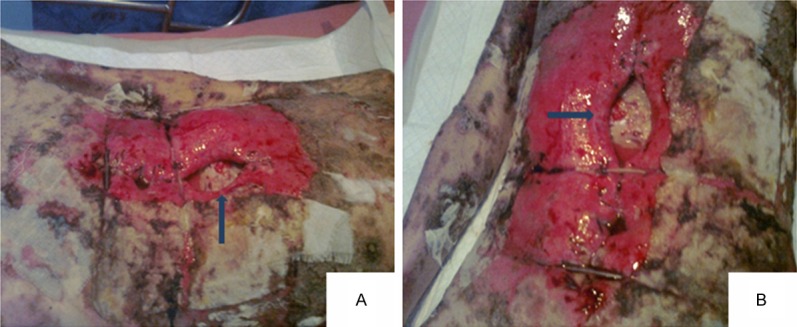
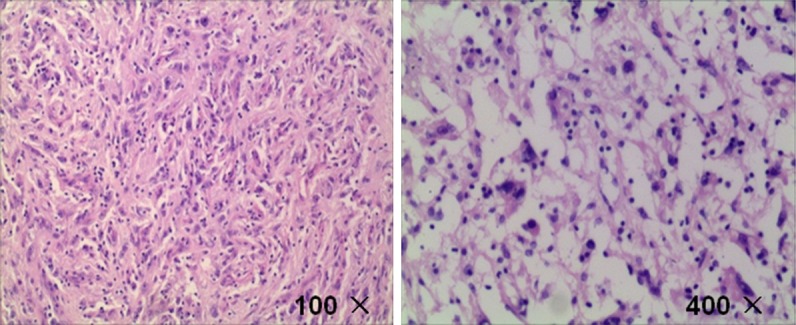
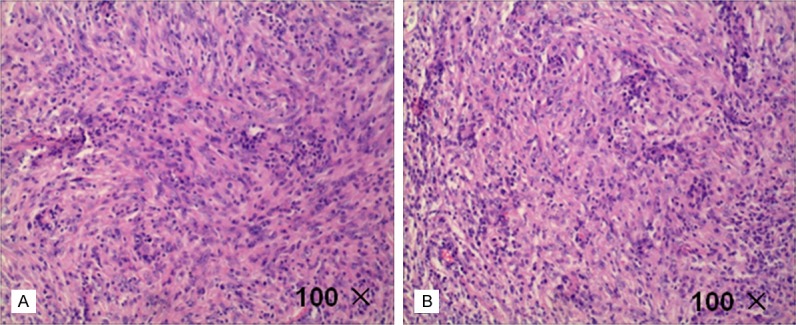
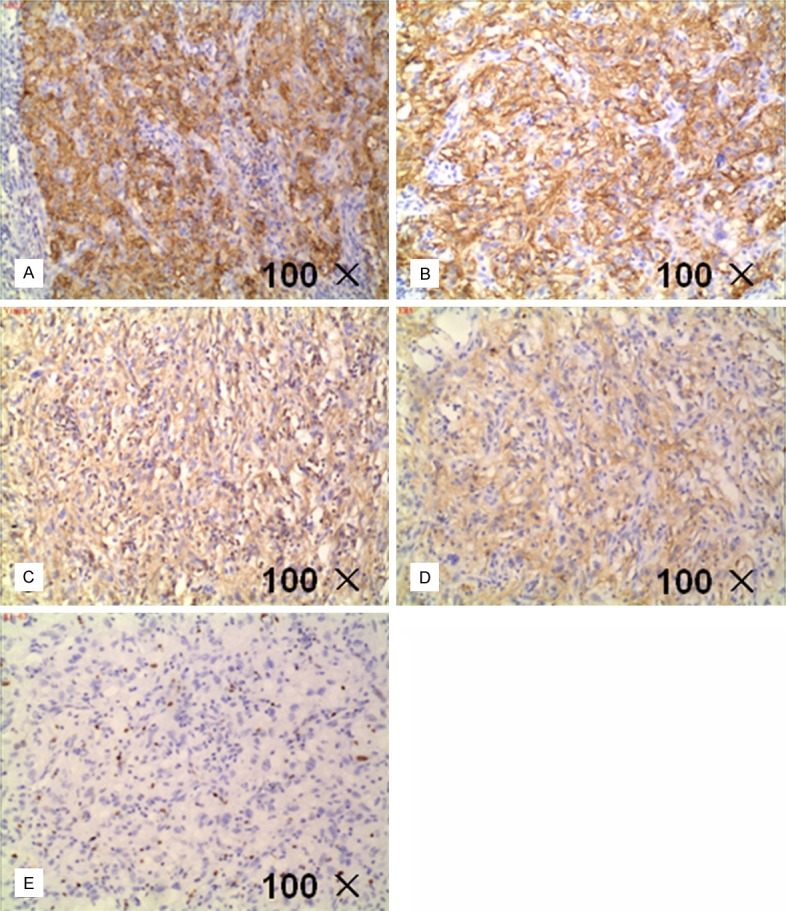
Follicular dendritic cell sarcoma (FDCS) is a rare tumor associated with paraneoplastic pemphigus. It is Blame drenchs auxiliary cell tumor which is derived from the peripheral lymphoid tissues. Throughout the world, several patients of paraneoplastic pemphigus associated follicular dendritic cell sarcoma were reported in the literature, but mostly originated from the neck lymph nodes, and extranodal origin of follicular dendritic sarcoma was rarely reported. Also, so far we have found that the malignant degree of all patients diagnosed with malignant tumors have been reported were low and after combined treatment of surgery, radiotherapy and chemotherapy, most of the prognosis was good. However, here we present a patient of paraneoplastic pemphigus associated with follicular dendritic cell sarcoma origined from outside of the lymph nodes and had high tumor malignant degree for its unclear cell boundaries, obvious atypia and mitoses and the patient's state became progressively deteriorate after operation.
Keywords: Paraneoplastic; follicular dendritic cell sarcoma; pemphigus.
Figures

Similar articles
-
Paraneoplastic pemphigus and myasthenia gravis as the first manifestations of a rare case of pancreatic follicular dendritic cell sarcoma: CT findings and review of literature.BMC Gastroenterol. 2019 Jun 14;19(1):92. doi: 10.1186/s12876-019-1008-y. BMC Gastroenterol. 2019. PMID: 31200650 Free PMC article. Review.
-
Mediastinal follicular dendritic cell sarcoma with paraneoplastic pemphigus.Asian Cardiovasc Thorac Ann. 2015 Jul;23(6):732-4. doi: 10.1177/0218492314561501. Epub 2014 Nov 17. Asian Cardiovasc Thorac Ann. 2015. PMID: 25406405
-
Paraneoplastic pemphigus as the first manifestation of follicular dendritic cell sarcoma.J Dtsch Dermatol Ges. 2014 Jan;12(1):68-71. doi: 10.1111/ddg.12179. Epub 2013 Oct 11. J Dtsch Dermatol Ges. 2014. PMID: 24119156 No abstract available.
-
Paraneoplastic pemphigus associated with primary pulmonar follicular dendritic cell sarcoma showing good response to treatment.J Eur Acad Dermatol Venereol. 2016 Mar;30(3):465-7. doi: 10.1111/jdv.12842. Epub 2014 Nov 11. J Eur Acad Dermatol Venereol. 2016. PMID: 25388966 No abstract available.
-
Clinical and pathological features of head and neck follicular dendritic cell sarcoma.Hematology. 2015 Dec;20(10):571-83. doi: 10.1179/1607845415Y.0000000008. Epub 2015 Apr 1. Hematology. 2015. PMID: 25831474 Review.
Cited by
-
Paraneoplastic pemphigus and myasthenia gravis as the first manifestations of a rare case of pancreatic follicular dendritic cell sarcoma: CT findings and review of literature.BMC Gastroenterol. 2019 Jun 14;19(1):92. doi: 10.1186/s12876-019-1008-y. BMC Gastroenterol. 2019. PMID: 31200650 Free PMC article. Review.
-
Clinicopathological characteristics of extranodal follicular dendritic cell sarcoma: A report of two cases.Oncol Lett. 2021 Mar;21(3):182. doi: 10.3892/ol.2021.12443. Epub 2021 Jan 6. Oncol Lett. 2021. PMID: 33574921 Free PMC article.
-
Intra-abdominal inflammatory pseudotumor-like follicular dendritic cell sarcoma associated with paraneoplastic pemphigus: A case report and review of the literature.World J Clin Cases. 2020 Jul 26;8(14):3097-3107. doi: 10.12998/wjcc.v8.i14.3097. World J Clin Cases. 2020. PMID: 32775392 Free PMC article.
-
Death within 9 months in patient with follicular dendritic cell sarcoma of spleen: A case report.Oncol Lett. 2022 Nov 21;25(1):15. doi: 10.3892/ol.2022.13601. eCollection 2023 Jan. Oncol Lett. 2022. PMID: 36478901 Free PMC article.
-
Follicular Dendritic Cell Sarcoma of Gastrointestinal Tract: an Uncommon Lesion, Commonly Missed.J Gastrointest Cancer. 2019 Dec;50(4):913-918. doi: 10.1007/s12029-018-0178-0. J Gastrointest Cancer. 2019. PMID: 30430359
References
-
- Urun Y, Kankaya D, Koral L, Yalcin B, Karabork A, Ceyhan K, Boruban MC, Utkan G, Demirkazik A. Intraabdominal follicular dendritic cell sarcoma: a report of three cases and review of the literature. Tumori. 2013;99:e65–69. - PubMed
-
- Choe JY, Go H, Jeon YK, Yun JY, Kim YA, Kim HJ, Huh J, Lee H, Shin DH, Kim JE. Inflammatory pseudotumor-like follicular dendritic cell sarcoma of the spleen: a report of six cases with increased IgG4-positive plasma cells. Pathol Int. 2013;63:245–251. - PubMed
-
- Perkins SM, Shinohara ET. Interdigitating and follicular dendritic cell sarcomas: a SEER analysis. Am J Clin Oncol. 2013;36:395–398. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials