

Endoscopic incisional therapy for benign esophageal strictures: Technique and results
- PMID: 26722613
- PMCID: PMC4689794
- DOI: 10.4253/wjge.v7.i19.1318
Endoscopic incisional therapy for benign esophageal strictures: Technique and results
Abstract
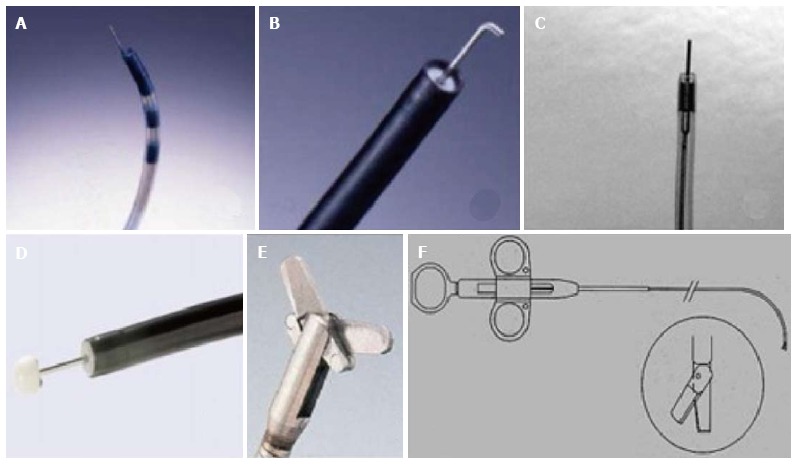
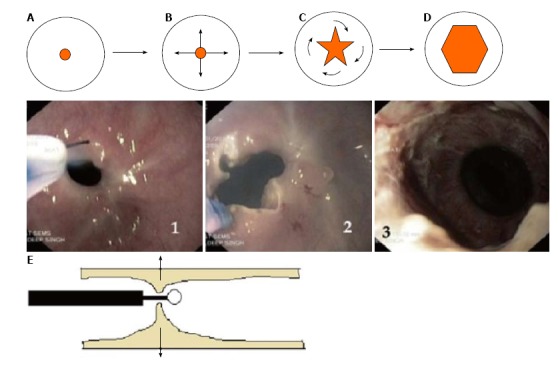
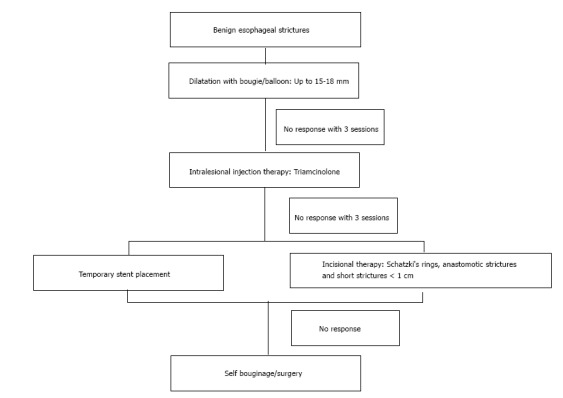
Benign esophageal strictures refractory to the conventional balloon or bougie dilatation may be subjected to various adjunctive modes of therapy, one of them being endoscopic incisional therapy (EIT). A proper delineation of the stricture anatomy is a prerequisite. A host of electrocautery and mechanical devices may be used, the most common being the use of needle knife, either standard or insulated tip. The technique entails radial incision and cutting off of the stenotic rim. Adjunctive therapies, to prevent re-stenosis, such as balloon dilatation, oral or intralesional steroids or argon plasma coagulation can be used. The common strictures where EIT has been successfully used are Schatzki's rings (SR) and anastomotic strictures (AS). Short segment strictures (< 1 cm) have been found to have the best outcome. When compared with routine balloon dilatation, EIT has equivalent results in treatment naïve cases but better long term outcome in refractory cases. Anecdotal reports of its use in other types of strictures have been noted. Post procedure complications of EIT are mild and comparable to dilatation therapy. As of the current evidence, incisional therapy can be used for management of refractory AS and SR with relatively short stenosis (< 1 cm) with good safety profile and acceptable long term patency.
Keywords: Anastomotic strictures; Endoscopic incisional therapy; Esophageal strictures; Needle knife; Radial incision and cutting.
Figures
Similar articles
-
Endoscopic Electrocautery Incisional Therapy as a Treatment for Refractory Benign Pediatric Esophageal Strictures.J Pediatr Gastroenterol Nutr. 2018 Oct;67(4):464-468. doi: 10.1097/MPG.0000000000002008. J Pediatr Gastroenterol Nutr. 2018. PMID: 29697549
-
Comparison of the Efficacy and Safety of Endoscopic Incisional Therapy and Balloon Dilatation for Esophageal Anastomotic Stricture.J Gastrointest Surg. 2021 Jul;25(7):1690-1695. doi: 10.1007/s11605-020-04811-3. Epub 2020 Oct 13. J Gastrointest Surg. 2021. PMID: 33051806
-
Primary incisional therapy with a modified method for patients with benign anastomotic esophageal stricture.Gastrointest Endosc. 2009 May;69(6):1029-33. doi: 10.1016/j.gie.2008.07.018. Epub 2009 Feb 11. Gastrointest Endosc. 2009. PMID: 19215919
-
Flexible endoscopic strategies for the difficult esophageal stricture.Curr Opin Gastroenterol. 2020 Sep;36(5):379-384. doi: 10.1097/MOG.0000000000000658. Curr Opin Gastroenterol. 2020. PMID: 32618615 Review.
-
Endoscopic treatment of benign esophageal strictures: a literature review.Expert Rev Gastroenterol Hepatol. 2017 Jan;11(1):53-64. doi: 10.1080/17474124.2017.1260002. Epub 2016 Nov 22. Expert Rev Gastroenterol Hepatol. 2017. PMID: 27835929 Review.
Cited by
-
A new simple endoscopic incision therapy for refractory benign oesophageal anastomotic stricture.BMJ Case Rep. 2021 Mar 10;14(3):e239798. doi: 10.1136/bcr-2020-239798. BMJ Case Rep. 2021. PMID: 33692055 Free PMC article.
-
Outcomes of Endoscopic Dilation in Patients with Esophageal Anastomotic Strictures: Comparison Between Different Etiologies.Dysphagia. 2020 Feb;35(1):73-83. doi: 10.1007/s00455-019-10004-1. Epub 2019 Mar 30. Dysphagia. 2020. PMID: 30929058
-
Safety and efficacy of coaxial lumen-apposing metal stents in the management of refractory gastrointestinal luminal strictures: a multicenter study.Endosc Int Open. 2017 Sep;5(9):E861-E867. doi: 10.1055/s-0043-114665. Epub 2017 Sep 12. Endosc Int Open. 2017. PMID: 28924591 Free PMC article.
-
Off label use of lumen-apposing metal stent for persistent gastro-jejunal anastomotic stricture.World J Gastrointest Endosc. 2018 Jun 16;10(6):117-120. doi: 10.4253/wjge.v10.i6.117. World J Gastrointest Endosc. 2018. PMID: 29988884 Free PMC article.
-
Management of ileocolic anastomotic strictures in Crohn's disease: endoscopic or surgical intervention? A systematic review and meta-analysis.Int J Colorectal Dis. 2025 Jul 24;40(1):162. doi: 10.1007/s00384-025-04958-y. Int J Colorectal Dis. 2025. PMID: 40707850 Free PMC article.
References
-
- Pasha SF, Acosta RD, Chandrasekhara V, Chathadi KV, Decker GA, Early DS, Evans JA, Fanelli RD, Fisher DA, Foley KQ, et al. The role of endoscopy in the evaluation and management of dysphagia. Gastrointest Endosc. 2014;79:191–201. - PubMed
-
- Lew RJ, Kochman ML. A review of endoscopic methods of esophageal dilation. J Clin Gastroenterol. 2002;35:117–126. - PubMed
-
- Pereira-Lima JC, Ramires RP, Zamin I, Cassal AP, Marroni CA, Mattos AA. Endoscopic dilation of benign esophageal strictures: report on 1043 procedures. Am J Gastroenterol. 1999;94:1497–1501. - PubMed
-
- Kochman ML, McClave SA, Boyce HW. The refractory and the recurrent esophageal stricture: a definition. Gastrointest Endosc. 2005;62:474–475. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
