

Role of Magnetic Resonance Imaging in Prostate Cancer Screening: A Pilot Study Within the Göteborg Randomised Screening Trial
- PMID: 26724840
- PMCID: PMC4958033
- DOI: 10.1016/j.eururo.2015.12.006
Role of Magnetic Resonance Imaging in Prostate Cancer Screening: A Pilot Study Within the Göteborg Randomised Screening Trial
Erratum in
-
Corrigendum re: "Role of Magnetic Resonance Imaging in Prostate Cancer Screening: A Pilot Study Within the Göteborg Randomised Screening Trial" [Eur Urol 2016;70:566-73].Eur Urol. 2017 Feb;71(2):e81. doi: 10.1016/j.eururo.2016.09.014. Epub 2016 Sep 20. Eur Urol. 2017. PMID: 27663047 No abstract available.
Abstract
Background: Magnetic resonance imaging (MRI) and targeted biopsies (TB) have shown potential to more accurately detect significant prostate cancer compared with prostate-specific antigen (PSA) and systematic biopsies (SB).
Objective: To compare sequential screening (PSA+MRI) with conventional PSA screening.
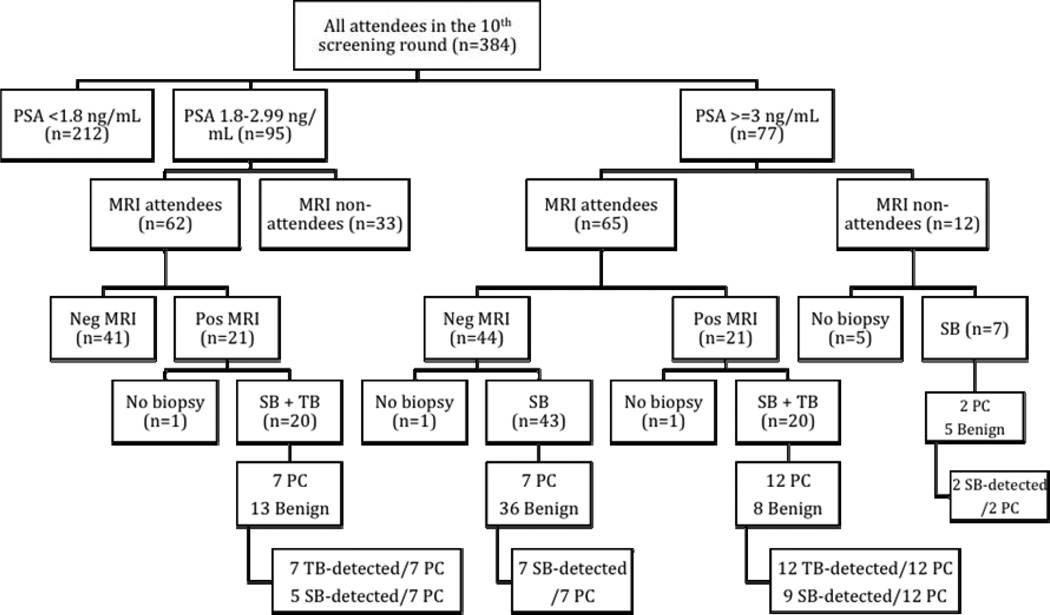
Design, setting, and participants: Of 384 attendees in the 10th screening round of the Göteborg randomised screening trial, 124 men, median age 69.5 yr, had a PSA of ≥ 1.8 ng/ml and underwent a prebiopsy MRI. Men with suspicious lesions on MRI and/or PSA ≥ 3.0ng/ml were referred for biopsy. SB was performed blinded to MRI results and TB was performed in men with tumour-suspicious findings on MRI. Three screening strategies were compared (PSA ≥ 3.0+SB; PSA ≥ 3.0+MRI+TB and PSA ≥ 1.8+MRI+TB).
Outcome measurements and statistical analysis: Cancer detection rates, sensitivity, and specificity were calculated per screening strategy and compared using McNemar's test.
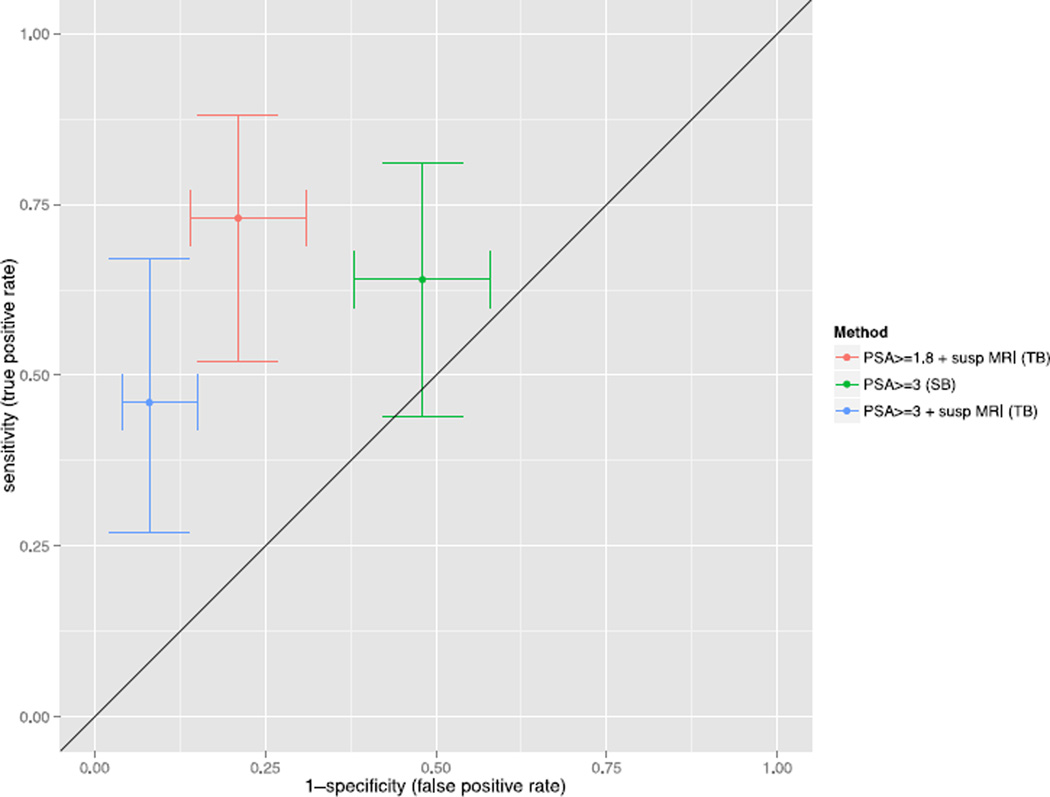
Results and limitations: In total, 28 cases of prostate cancer were detected, of which 20 were diagnosed in biopsy-naïve men. Both PSA ≥ 3.0+MRI and PSA ≥ 1.8+MRI significantly increased specificity compared with PSA ≥ 3.0+SB (0.92 and 0.79 vs 0.52; p<0.002 for both), while sensitivity was significantly higher for PSA ≥ 1.8+MRI compared with PSA ≥ 3.0+MRI (0.73 vs 0.46, p=0.008). The detection rate of significant cancer was higher with PSA ≥ 1.8+MRI compared with PSA ≥ 3.0+SB (5.9% vs 4.0%), while the detection rate of insignificant cancer was lowered by PSA ≥ 3.0+MRI (0.3% vs 1.2%). The primary limitation of this study is the small sample of men.
Conclusion: A screening strategy with a lowered PSA cut-off followed by TB in MRI-positive men seems to increase the detection of significant cancers while improving specificity. If replicated, these results may contribute to a paradigm shift in future screening.
Patient summary: Major concerns in prostate-specific antigen screening are overdiagnosis and underdiagnosis. We evaluated whether prostate magnetic resonance imaging could improve the balance of benefits to harm in prostate cancer screening screening, and we found a promising potential of using magnetic resonance imaging in addition to prostate-specific antigen.
Keywords: Imaging; MRI; PSA screening; Prostate cancer.
Copyright © 2015 European Association of Urology. Published by Elsevier B.V. All rights reserved.
Figures
Comment in
-
The Role of Magnetic Resonance Imaging in Prostate Cancer: Focusing on What Really Matters.Eur Urol. 2016 Oct;70(4):574-575. doi: 10.1016/j.eururo.2016.01.039. Epub 2016 Feb 6. Eur Urol. 2016. PMID: 26861475 No abstract available.
References
-
- Thompson IM, Ankerst DP, Chi C, et al. Operating characteristics of prostate-specific antigen in men with an initial PSA level of 3.0 ng/ml or lower. JAMA : the journal of the American Medical Association. 2005;294(1):66–70. - PubMed
-
- Bak JB, Landas SK, Haas GP. Characterization of prostate cancer missed by sextant biopsy. Clinical prostate cancer. 2003;2(2):115–118. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
