

Total Serum Bilirubin within 3 Months of Hepatoportoenterostomy Predicts Short-Term Outcomes in Biliary Atresia
- PMID: 26725209
- PMCID: PMC4826612
- DOI: 10.1016/j.jpeds.2015.11.058
Total Serum Bilirubin within 3 Months of Hepatoportoenterostomy Predicts Short-Term Outcomes in Biliary Atresia
Abstract
Objectives: To prospectively assess the value of serum total bilirubin (TB) within 3 months of hepatoportoenterostomy (HPE) in infants with biliary atresia as a biomarker predictive of clinical sequelae of liver disease in the first 2 years of life.
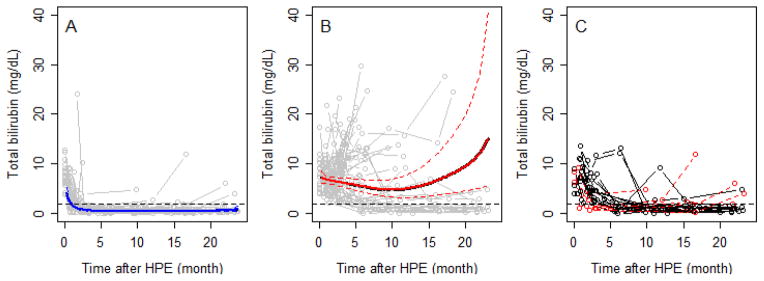
Study design: Infants with biliary atresia undergoing HPE between June 2004 and January 2011 were enrolled in a prospective, multicenter study. Complications were monitored until 2 years of age or the earliest of liver transplantation (LT), death, or study withdrawal. TB below 2 mg/dL (34.2 μM) at any time in the first 3 months (TB <2.0, all others TB ≥ 2) after HPE was examined as a biomarker, using Kaplan-Meier survival and logistic regression.
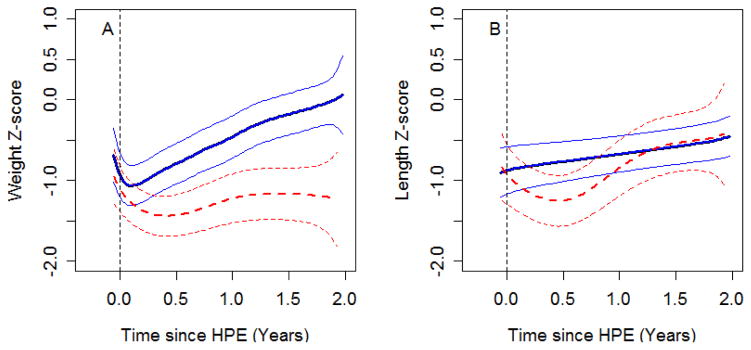
Results: Fifty percent (68/137) of infants had TB < 2.0 in the first 3 months after HPE. Transplant-free survival at 2 years was significantly higher in the TB < 2.0 group vs TB ≥ 2 (86% vs 20%, P < .0001). Infants with TB ≥ 2 had diminished weight gain (P < .0001), greater probability of developing ascites (OR 6.4, 95% CI 2.9-14.1, P < .0001), hypoalbuminemia (OR 7.6, 95% CI 3.2-17.7, P < .0001), coagulopathy (OR 10.8, 95% CI 3.1-38.2, P = .0002), LT (OR 12.4, 95% CI 5.3-28.7, P < .0001), or LT or death (OR 16.8, 95% CI 7.2-39.2, P < .0001).
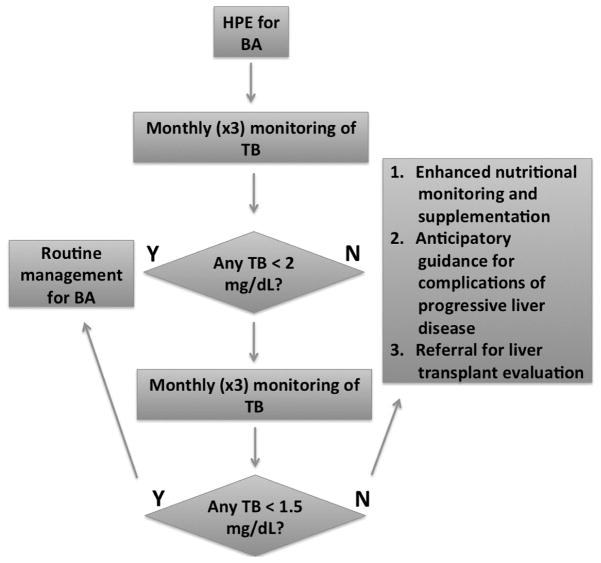
Conclusions: Infants whose TB does not fall below 2.0 mg/dL within 3 months of HPE were at high risk for early disease progression, suggesting they should be considered for LT in a timely fashion. Interventions increasing the likelihood of achieving TB <2.0 mg/dL within 3 months of HPE may enhance early outcomes.
Trial registration: ClinicalTrials.gov: NCT00061828 and NCT00294684.
Copyright © 2016 Elsevier Inc. All rights reserved.
Figures

References
-
- Kasai M, Kimura S, Asakura Y, Suzuki H, Taira Y, Ohashi E. Surgical treatment of biliary atresia. J Pediatr Surg. 1968;3:665–75.
-
- Davenport M, Caponcelli E, Livesey E, Hadzic N, Howard E. Surgical outcome in biliary atresia: etiology affects the influence of age at surgery. Ann Surg. 2008;247:694–8. - PubMed
-
- Wildhaber BE, Coran AG, Drongowski RA, Hirschl RB, Geiger JD, Lelli JL, et al. The Kasai portoenterostomy for biliary atresia: A review of a 27-year experience with 81 patients. J Pediatr Surg. 2003;38:1480–5. - PubMed
-
- Valayer J. Conventional treatment of biliary atresia: long-term results. J Pediatr Surg. 1996;31:1546–51. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- U01DK062452/DK/NIDDK NIH HHS/United States
- U01 DK062481/DK/NIDDK NIH HHS/United States
- U01DK062500/DK/NIDDK NIH HHS/United States
- UL1TR000423/TR/NCATS NIH HHS/United States
- UL1TR000454/TR/NCATS NIH HHS/United States
- U01 DK062470/DK/NIDDK NIH HHS/United States
- UL1TR000150/TR/NCATS NIH HHS/United States
- UL1TR001082/TR/NCATS NIH HHS/United States
- U01 DK103140/DK/NIDDK NIH HHS/United States
- U01DK084536/DK/NIDDK NIH HHS/United States
- U01DK062503/DK/NIDDK NIH HHS/United States
- U01 DK084538/DK/NIDDK NIH HHS/United States
- U01 DK062453/DK/NIDDK NIH HHS/United States
- P30 DK026743/DK/NIDDK NIH HHS/United States
- U01 DK062503/DK/NIDDK NIH HHS/United States
- P30 DK078392/DK/NIDDK NIH HHS/United States
- U01 DK103135/DK/NIDDK NIH HHS/United States
- U01DK062453/DK/NIDDK NIH HHS/United States
- UL1TR001108/TR/NCATS NIH HHS/United States
- U01DK084575/DK/NIDDK NIH HHS/United States
- U01 DK062436/DK/NIDDK NIH HHS/United States
- UL1TR000005/TR/NCATS NIH HHS/United States
- U01DK062466/DK/NIDDK NIH HHS/United States
- U01 DK062452/DK/NIDDK NIH HHS/United States
- U01 DK062466/DK/NIDDK NIH HHS/United States
- UL1TR000077/TR/NCATS NIH HHS/United States
- U01DK062470/DK/NIDDK NIH HHS/United States
- UL1TR000448/TR/NCATS NIH HHS/United States
- UL1RR025014/RR/NCRR NIH HHS/United States
- U01 DK084575/DK/NIDDK NIH HHS/United States
- UL1 TR000454/TR/NCATS NIH HHS/United States
- U01DK062481/DK/NIDDK NIH HHS/United States
- U01DK062436/DK/NIDDK NIH HHS/United States
- UL1TR000004/TR/NCATS NIH HHS/United States
- U01 DK084536/DK/NIDDK NIH HHS/United States
- UL1 TR000448/TR/NCATS NIH HHS/United States
- U01DK103149/DK/NIDDK NIH HHS/United States
- UL1TR000130/TR/NCATS NIH HHS/United States
- UL1 TR001425/TR/NCATS NIH HHS/United States
- U01DK084538/DK/NIDDK NIH HHS/United States
- UL1 TR002319/TR/NCATS NIH HHS/United States
- UL1 TR001082/TR/NCATS NIH HHS/United States
- U01 DK062456/DK/NIDDK NIH HHS/United States
- U01DK103135/DK/NIDDK NIH HHS/United States
- U01 DK062445/DK/NIDDK NIH HHS/United States
- U01 DK103149/DK/NIDDK NIH HHS/United States
- UL1TR000424/TR/NCATS NIH HHS/United States
- U01DK062497/DK/NIDDK NIH HHS/United States
- U01DK062445/DK/NIDDK NIH HHS/United States
- U01 DK062500/DK/NIDDK NIH HHS/United States
- U01 DK062497/DK/NIDDK NIH HHS/United States
- U01DK062456/DK/NIDDK NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
