

Exploratory Study of 4D versus 3D Robust Optimization in Intensity Modulated Proton Therapy for Lung Cancer
- PMID: 26725727
- PMCID: PMC4834263
- DOI: 10.1016/j.ijrobp.2015.11.002
Exploratory Study of 4D versus 3D Robust Optimization in Intensity Modulated Proton Therapy for Lung Cancer
Abstract
Purpose: The purpose of this study was to compare the impact of uncertainties and interplay on 3-dimensional (3D) and 4D robustly optimized intensity modulated proton therapy (IMPT) plans for lung cancer in an exploratory methodology study.
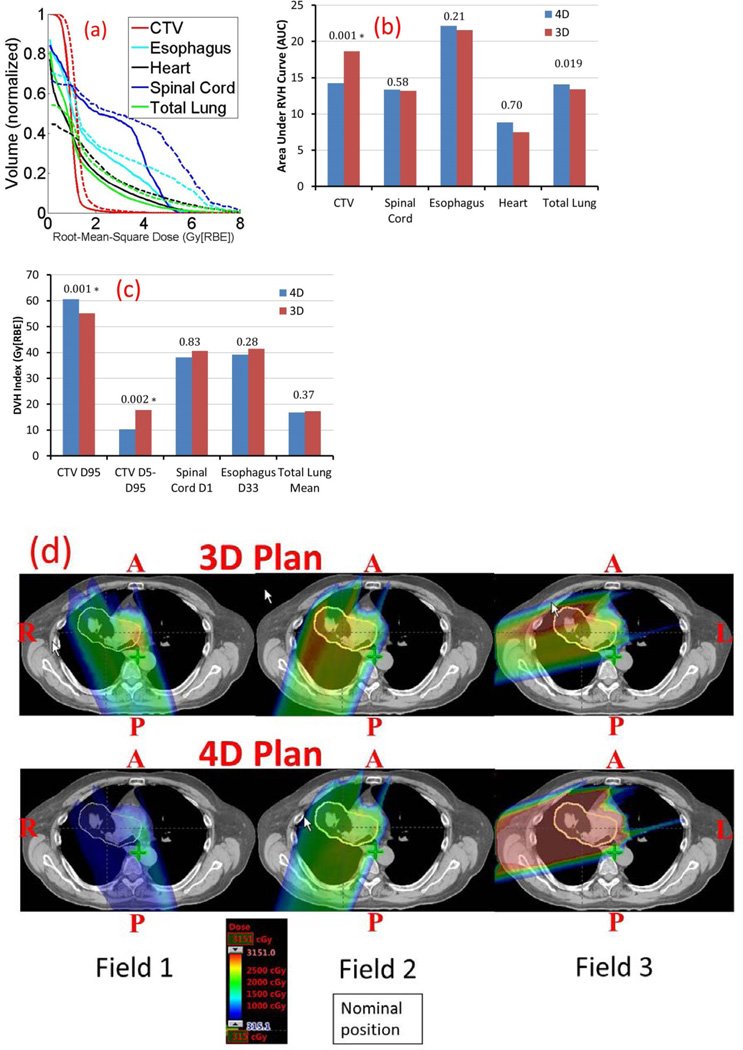
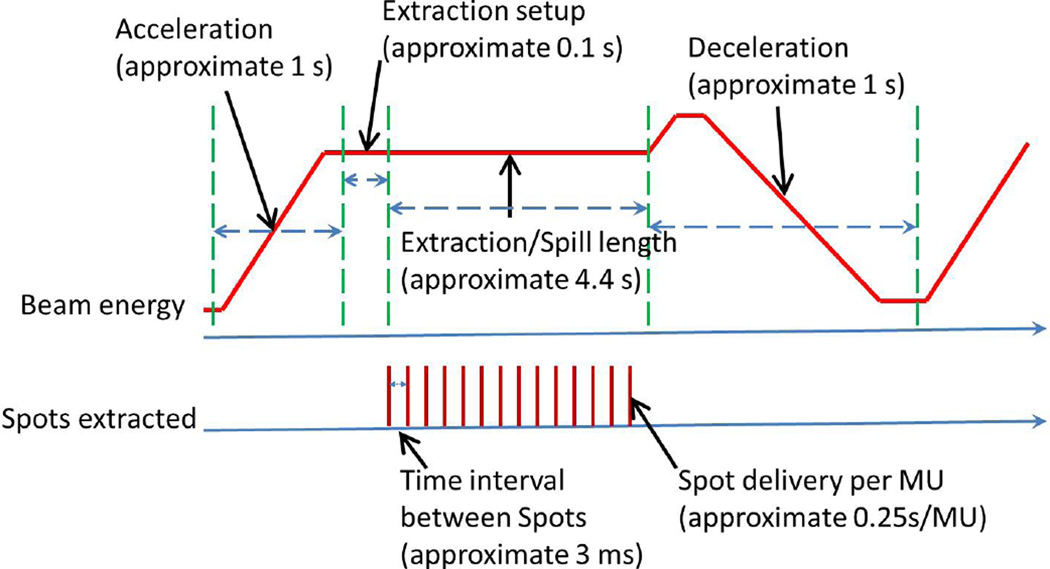
Methods and materials: IMPT plans were created for 11 nonrandomly selected non-small cell lung cancer (NSCLC) cases: 3D robustly optimized plans on average CTs with internal gross tumor volume density overridden to irradiate internal target volume, and 4D robustly optimized plans on 4D computed tomography (CT) to irradiate clinical target volume (CTV). Regular fractionation (66 Gy [relative biological effectiveness; RBE] in 33 fractions) was considered. In 4D optimization, the CTV of individual phases received nonuniform doses to achieve a uniform cumulative dose. The root-mean-square dose-volume histograms (RVH) measured the sensitivity of the dose to uncertainties, and the areas under the RVH curve (AUCs) were used to evaluate plan robustness. Dose evaluation software modeled time-dependent spot delivery to incorporate interplay effect with randomized starting phases of each field per fraction. Dose-volume histogram (DVH) indices comparing CTV coverage, homogeneity, and normal tissue sparing were evaluated using Wilcoxon signed rank test.
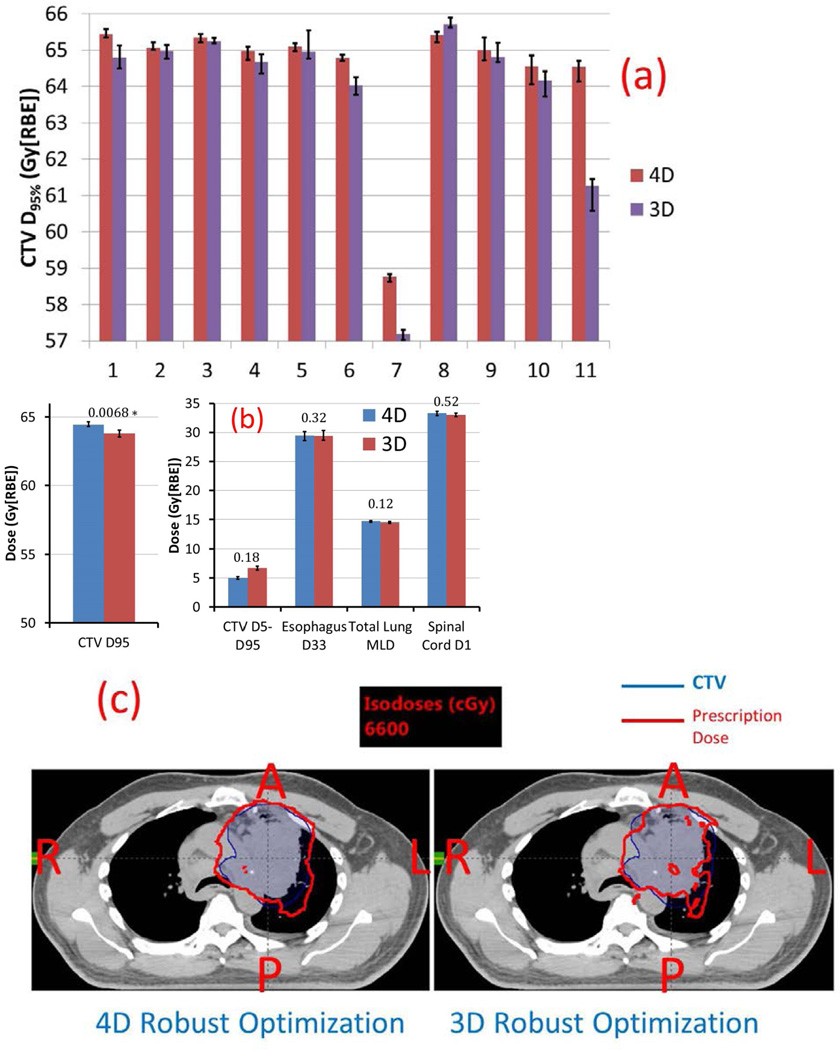
Results: 4D robust optimization plans led to smaller AUC for CTV (14.26 vs 18.61, respectively; P=.001), better CTV coverage (Gy [RBE]) (D95% CTV: 60.6 vs 55.2, respectively; P=.001), and better CTV homogeneity (D5%-D95% CTV: 10.3 vs 17.7, respectively; P=.002) in the face of uncertainties. With interplay effect considered, 4D robust optimization produced plans with better target coverage (D95% CTV: 64.5 vs 63.8, respectively; P=.0068), comparable target homogeneity, and comparable normal tissue protection. The benefits from 4D robust optimization were most obvious for the 2 typical stage III lung cancer patients.
Conclusions: Our exploratory methodology study showed that, compared to 3D robust optimization, 4D robust optimization produced significantly more robust and interplay-effect-resistant plans for targets with comparable dose distributions for normal tissues. A further study with a larger and more realistic patient population is warranted to generalize the conclusions.
Copyright © 2016 Elsevier Inc. All rights reserved.
Conflict of interest statement
None
Figures
Similar articles
-
Technical Note: Treatment planning system (TPS) approximations matter - comparing intensity-modulated proton therapy (IMPT) plan quality and robustness between a commercial and an in-house developed TPS for nonsmall cell lung cancer (NSCLC).Med Phys. 2019 Nov;46(11):4755-4762. doi: 10.1002/mp.13809. Epub 2019 Sep 21. Med Phys. 2019. PMID: 31498885
-
Impact of Spot Size and Spacing on the Quality of Robustly Optimized Intensity Modulated Proton Therapy Plans for Lung Cancer.Int J Radiat Oncol Biol Phys. 2018 Jun 1;101(2):479-489. doi: 10.1016/j.ijrobp.2018.02.009. Epub 2018 Feb 14. Int J Radiat Oncol Biol Phys. 2018. PMID: 29550033 Free PMC article.
-
Intensity-modulated proton therapy (IMPT) interplay effect evaluation of asymmetric breathing with simultaneous uncertainty considerations in patients with non-small cell lung cancer.Med Phys. 2020 Nov;47(11):5428-5440. doi: 10.1002/mp.14491. Epub 2020 Oct 13. Med Phys. 2020. PMID: 32964474 Free PMC article.
-
Robust optimization in lung treatment plans accounting for geometric uncertainty.J Appl Clin Med Phys. 2018 May;19(3):19-26. doi: 10.1002/acm2.12291. Epub 2018 Mar 10. J Appl Clin Med Phys. 2018. PMID: 29524301 Free PMC article. Review.
-
Consensus Statement on Proton Therapy in Early-Stage and Locally Advanced Non-Small Cell Lung Cancer.Int J Radiat Oncol Biol Phys. 2016 May 1;95(1):505-516. doi: 10.1016/j.ijrobp.2016.01.036. Epub 2016 Jan 23. Int J Radiat Oncol Biol Phys. 2016. PMID: 27084663 Free PMC article. Review.
Cited by
-
Online adaptive dose restoration in intensity modulated proton therapy of lung cancer to account for inter-fractional density changes.Phys Imaging Radiat Oncol. 2020 Jul 13;15:30-37. doi: 10.1016/j.phro.2020.06.004. eCollection 2020 Jul. Phys Imaging Radiat Oncol. 2020. PMID: 33458323 Free PMC article.
-
Emerging technologies for cancer therapy using accelerated particles.Prog Part Nucl Phys. 2023 Jul;131:104046. doi: 10.1016/j.ppnp.2023.104046. Prog Part Nucl Phys. 2023. PMID: 37207092 Free PMC article.
-
Dosimetric comparison of distal esophageal carcinoma plans for patients treated with small-spot intensity-modulated proton versus volumetric-modulated arc therapies.J Appl Clin Med Phys. 2019 Jul;20(7):15-27. doi: 10.1002/acm2.12623. Epub 2019 May 21. J Appl Clin Med Phys. 2019. PMID: 31112371 Free PMC article.
-
On the pitfalls of PTV in lung SBRT using type-B dose engine: an analysis of PTV and worst case scenario concepts for treatment plan optimization.Radiat Oncol. 2020 May 29;15(1):130. doi: 10.1186/s13014-020-01573-9. Radiat Oncol. 2020. PMID: 32471457 Free PMC article.
-
Managing treatment-related uncertainties in proton beam radiotherapy for gastrointestinal cancers.J Gastrointest Oncol. 2020 Feb;11(1):212-224. doi: 10.21037/jgo.2019.11.07. J Gastrointest Oncol. 2020. PMID: 32175124 Free PMC article. Review.
References
-
- Zhang XD, Li YP, Pan XN, et al. Intensity-modulated proton therapy reduces the dose to normal tissue compared with intensity-modulated radiation therapy or passive scattering proton therapy and enables individualized radical radiotherapy for extensive stage IIIB non-small-cell lung cancer: a virtual clinical study. International Journal of Radiation Oncology Biology Physics. 2010;77:357–366. - PMC - PubMed
-
- Stuschke M, Kaiser A, Pottgen C, et al. Potentials of robust intensity modulated scanning proton plans for locally advanced lung cancer in comparison to intensity modulated photon plans. Radiotherapy and oncology : journal of the European Society for Therapeutic Radiology and Oncology. 2012;104:45–51. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
