

The incidence, mortality and timing of Pneumocystis jiroveci pneumonia after hematopoietic cell transplantation: a CIBMTR analysis
- PMID: 26726945
- PMCID: PMC4823157
- DOI: 10.1038/bmt.2015.316
The incidence, mortality and timing of Pneumocystis jiroveci pneumonia after hematopoietic cell transplantation: a CIBMTR analysis
Abstract
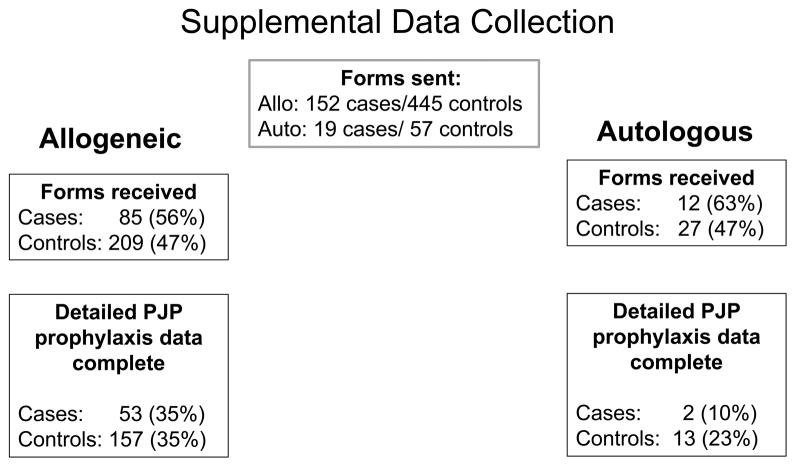
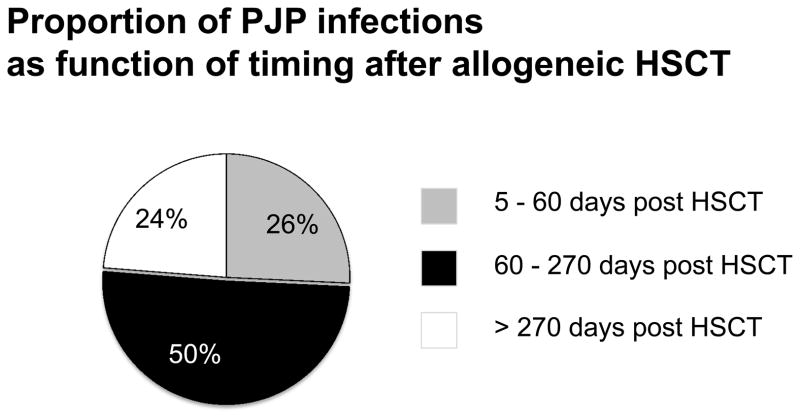
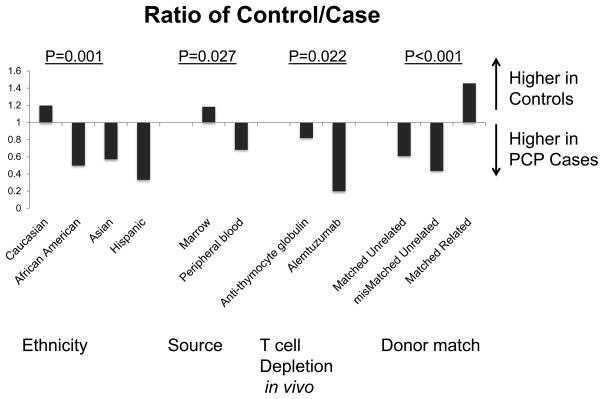
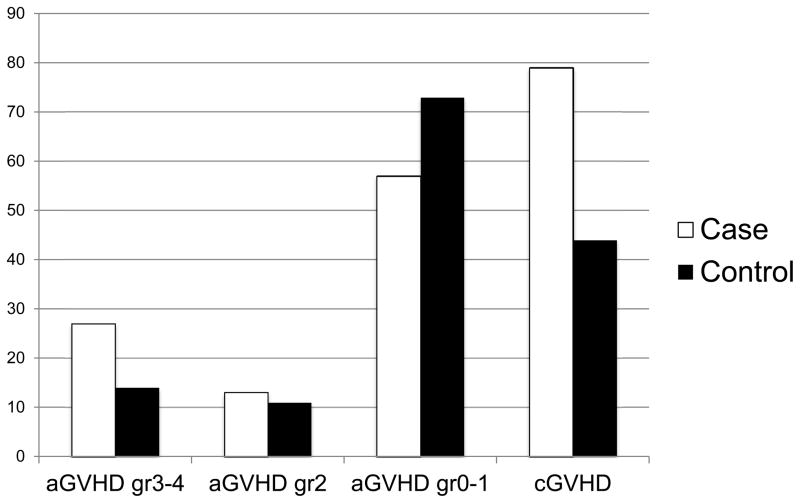
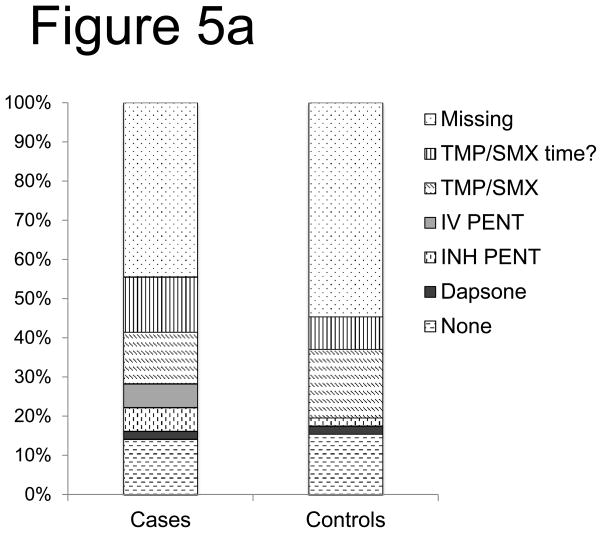
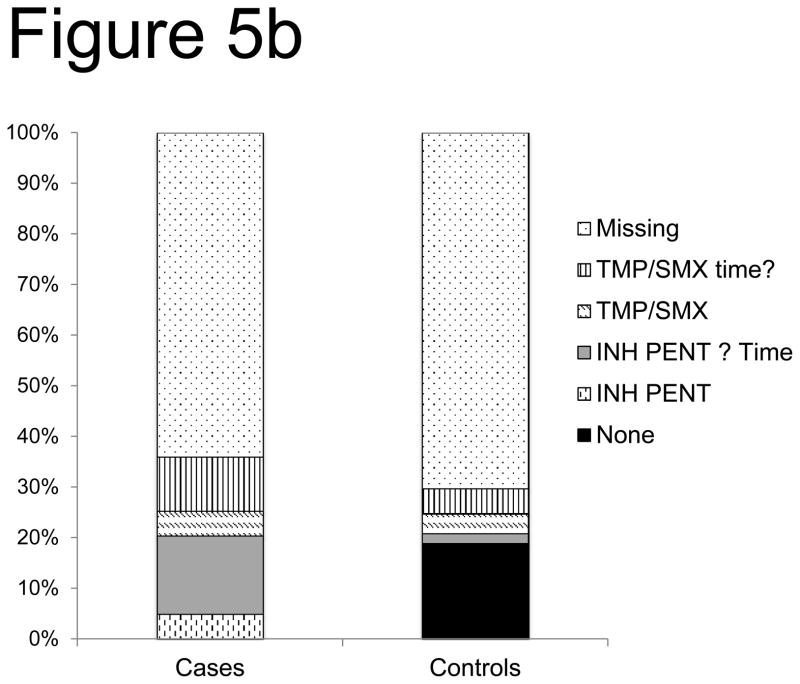
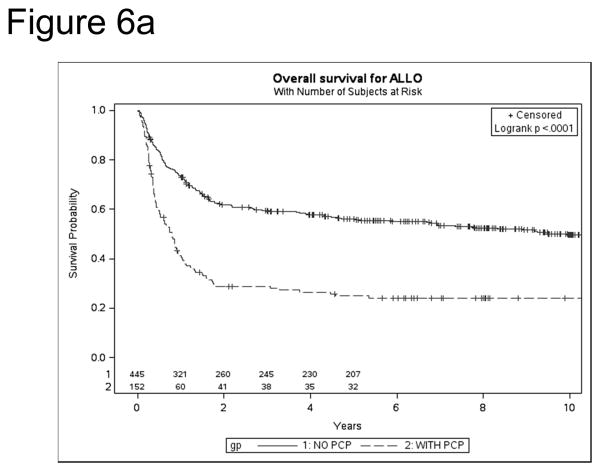
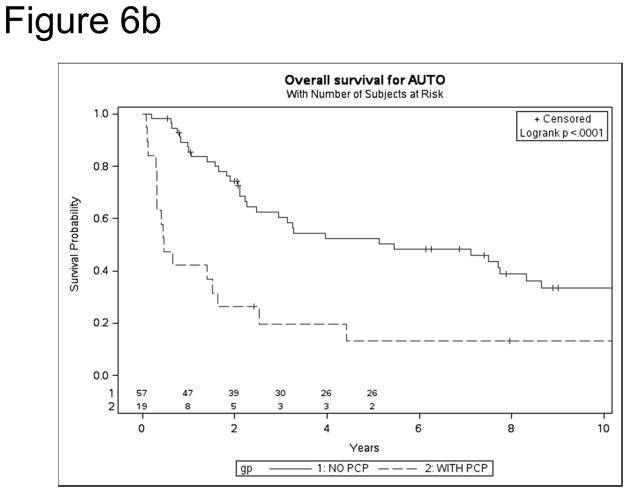
Pneumocystis jiroveci pneumonia (PJP) is associated with high morbidity and mortality after hematopoietic stem cell transplantation (HSCT). Little is known about PJP infections after HSCT because of the rarity of disease given routine prophylaxis. We report the results of a Center for International Blood and Marrow Transplant Research study evaluating the incidence, timing, prophylaxis agents, risk factors and mortality of PJP after autologous (auto) and allogeneic (allo) HSCT. Between 1995 and 2005, 0.63% allo recipients and 0.28% auto recipients of first HSCT developed PJP. Cases occurred as early as 30 days to beyond a year after allo HSCT. A nested case cohort analysis with supplemental data (n=68 allo cases, n=111 allo controls) revealed that risk factors for PJP infection included lymphopenia and mismatch after HSCT. After allo or auto HSCT, overall survival was significantly poorer among cases vs controls (P=0.0004). After controlling for significant variables, the proportional hazards model revealed that PJP cases were 6.87 times more likely to die vs matched controls (P<0.0001). We conclude PJP infection is rare after HSCT but is associated with high mortality. Factors associated with GVHD and with poor immune reconstitution are among the risk factors for PJP and suggest that protracted prophylaxis for PJP in high-risk HSCT recipients may improve outcomes.
Conflict of interest statement
Conflict of Interest Statement: There are no relevant conflicts of interest to disclose.
Figures
References
-
- Gilroy SA, Bennett NJ. Pneumocystis pneumonia. Seminars in Respiratory and Critical Care Medicine. 2011;32(6):775–782. - PubMed
-
- Wakefield AE, Peters SE, Banerji S, Bridge PD, Hall GS, Hawksworth DL, et al. Pneumocystis carinii shows DNA homology with the ustomycetous red yeast fungi. Molecular Microbiology. 1992;6(14):1903–1911. - PubMed
-
- Gluck T, Geerdes-Fenge HF, Straub RH, Raffenberg M, Lang B, Lode H, et al. Pneumocystis carinii pneumonia as a complication of immunosuppressive therapy. Infection. 2000;28(4):227–230. - PubMed
-
- Tuan IZ, Dennison D, Weisdorf DJ. Pneumocystis carinii pneumonitis following bone marrow transplantation. Bone Marrow Transplantation. 1992;10(3):267–272. - PubMed
-
- Wazir JF, Ansari NA. Pneumocystis carinii infection. Update and review Archives of Pathology & Laboratory Medicine. 2004;128(9):1023–1027. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
