

Comparison of linear motion perception thresholds in vestibular migraine and Menière's disease
- PMID: 26728484
- PMCID: PMC5014886
- DOI: 10.1007/s00405-015-3835-y
Comparison of linear motion perception thresholds in vestibular migraine and Menière's disease
Abstract
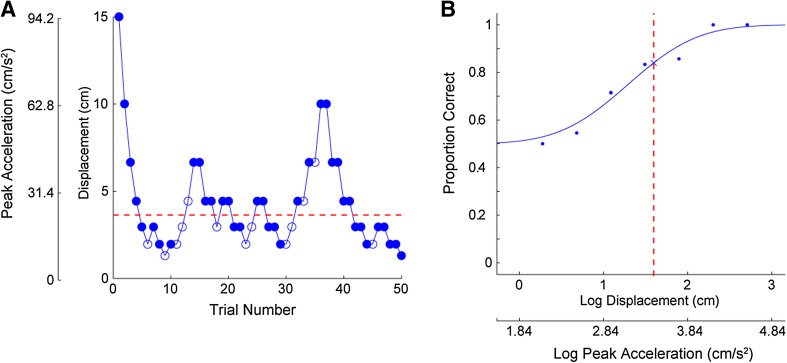
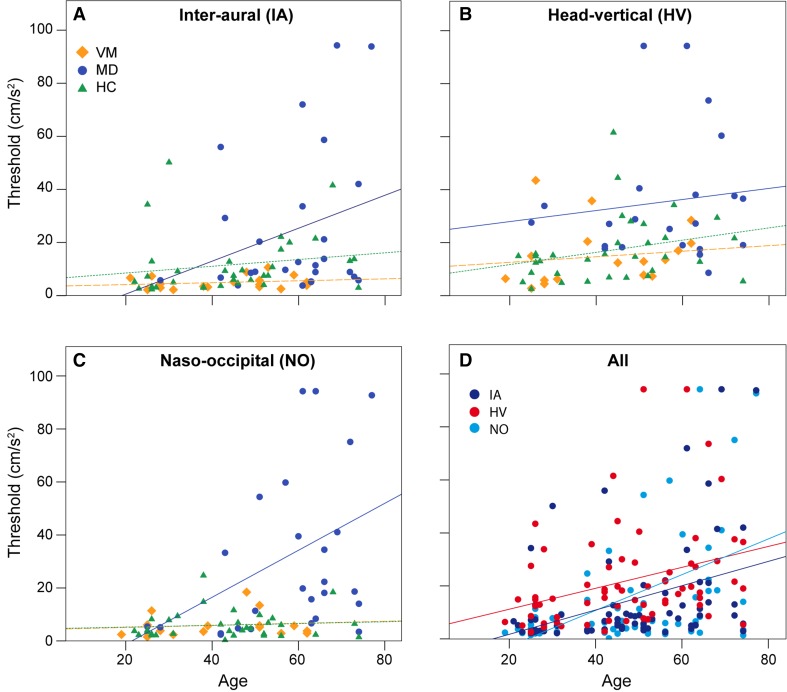
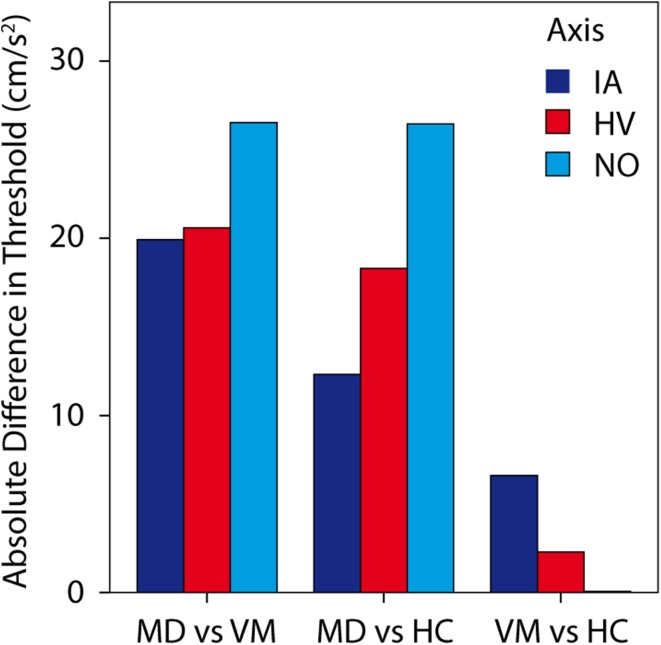
Linear motion perceptual thresholds (PTs) were compared between patients with Menière's disease (MD) and vestibular migraine (VM). Twenty patients with VM, 27 patients with MD and 34 healthy controls (HC) were examined. PTs for linear motion along the inter-aural (IA), naso-occipital axes (NO), and head-vertical (HV) axis were measured using a multi-axis motion platform. Ocular and cervical vestibular evoked myogenic potentials (o/c VEMP) were performed and the dizziness handicap inventory (DHI) administered. In order to discriminate between VM and MD, we also evaluated the diagnostic accuracy of applied methods. PTs depended significantly on the group tested (VM, MD and HC), as revealed by ANCOVA with group as the factor and age as the covariate. This was true for all motion axes (IA, HV and NO). Thresholds were highest for MD patients, significantly higher than for all other groups for all motion axes, except for the IA axis when compared with HC group suggesting decreased otolith sensitivity in MD patients. VM patients had thresholds that were not different from those of HC, but were significantly lower than those of the MD group for all motion axes. The cVEMP p13 latencies differed significantly across groups being lowest in VM. There was a statistically significant association between HV and NO thresholds and cVEMP PP amplitudes. Diagnostic accuracy was highest for the IA axis, followed by cVEMP PP amplitudes, NO and HV axes. To conclude, patients with MD had significantly higher linear motion perception thresholds compared to patients with VM and controls. Except for reduced cVEMP latency, there were no differences in c/oVEMP between MD, VM and controls.
Keywords: Diagnostic accuracy; Menière’s disease; Otolith function; Perception thresholds; Saccule; Utricle; Vestibular migraine.
Conflict of interest statement
T. Bremova and N. Böttcher received honoraria for lecturing from Actelion. A. Caushaj, M. Ertl, P. MacNeilage, R. Strobl report no disclosures. M. Strupp is Joint Chief Editor of the Journal of Neurology, Editor in Chief of Frontiers of Neuro-otology and Section Editor of F1000. He has received speaker’s honoraria from Abbott, Actelion, Biogen, Eisai, GSK, Henning Pharma, Interacoustics, MSD, Otometrics, Pierre-Fabre, TEVA, UCB. He acts as a consultant for Abbott and Actelion. Study funding Supported by German Ministry of Education and Research grant code 01 EO 0901 to the German Center for Vertigo and Balance Disorders at the University of Munich, Campus Großhadern.
Figures
References
-
- Lempert T, Olesen J, Furman J, et al. Vestibular migraine: diagnostic criteria. J Vestib Res Equilib Orientat. 2012;22:167–172. - PubMed
-
- Lopez-Escamez JA, Carey J, Chung W-H, et al. Diagnostic criteria for Menière’s disease. J Vestib Res Equilib Orientat. 2015;25:1–7. - PubMed
-
- Gürkov R, Flatz W, Louza J, et al. In vivo visualized endolymphatic hydrops and inner ear functions in patients with electrocochleographically confirmed Menière’s disease. Otol Neurotol Off Publ Am Otol Soc Am Neurotol Soc Eur Acad Otol Neurotol. 2012;33:1040–1045. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
