

Determinants of chronic obstructive pulmonary disease severity in the late-elderly differ from those in younger patients
- PMID: 26728686
- PMCID: PMC4700610
- DOI: 10.1186/s13104-015-1810-8
Determinants of chronic obstructive pulmonary disease severity in the late-elderly differ from those in younger patients
Abstract
Background: Although the age range of chronic obstructive pulmonary disease (COPD) patients is broad, few studies have focused on the effects of age on disease characteristics.
Methods: Keio University and affiliated hospitals established an observational COPD cohort. Patients were assessed using high resolution computed tomography (CT) to quantify emphysema, health status using the COPD assessment test (CAT) and the St. George's Respiratory Questionnaire (SGRQ), spirometry, echocardiogram, dual X-ray absorption of bone, biomarkers and comorbid diagnoses. We examined the characteristics of COPD patients aged 75 and over compared with patients below 75.
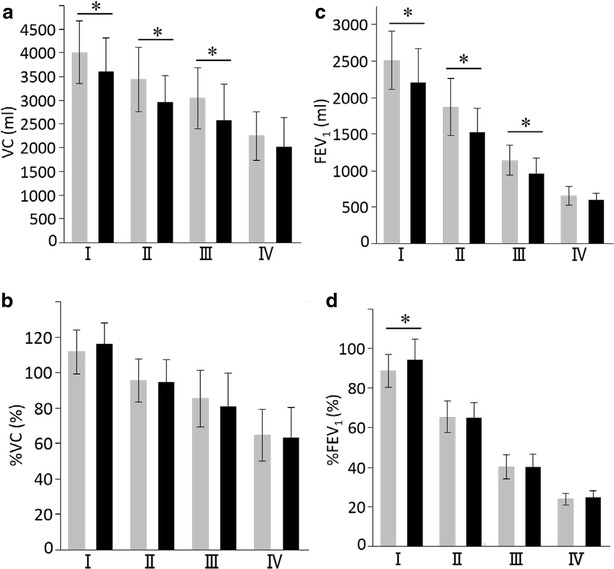
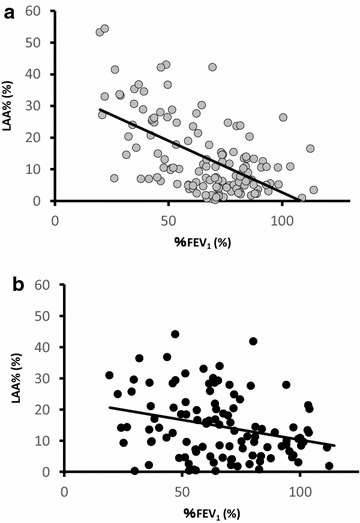
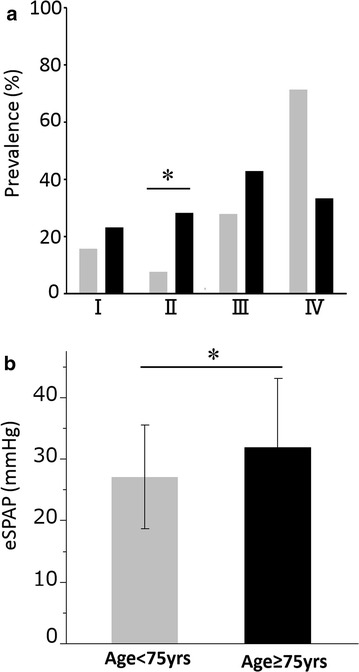
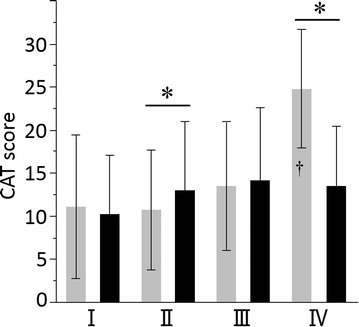
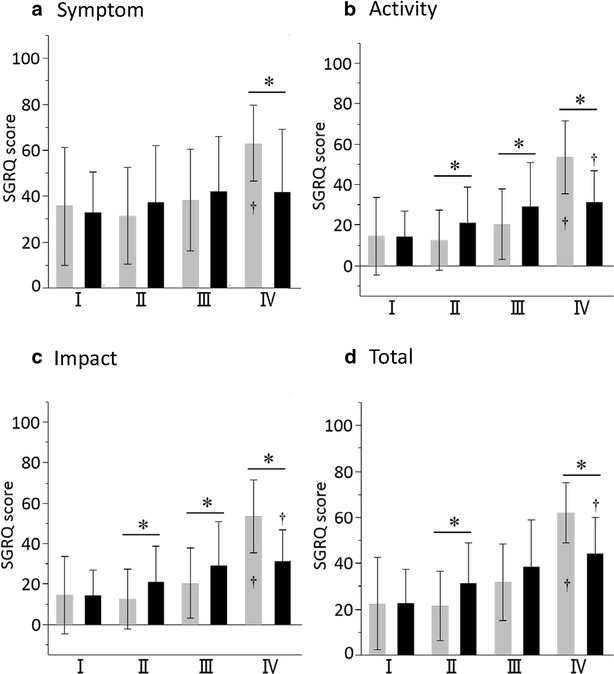
Results: A total of 443 patients comprising 252 patients aged <75 years and 191 patients aged ≥75 years, were enrolled. Emphysematous changes on CT and prevalence of possible pulmonary hypertension were greater in late-elderly patients. The slope of the relationship between CT emphysema densitometry score and forced expiratory volume in 1 s was significantly less steep in the late-elderly than the younger patients (p = 0.002). CAT and total SGRQ scores and the frequency of long-term oxygen therapy were significantly higher in the late-elderly with moderate airflow obstruction compared to those of the younger in the same grade, although the opposite was seen in late-elderly patients with very severe airflow obstruction. Hypertension, aortic aneurysm, prostatic hypertrophy, anemia, and cataract are more prevalent in late-elderly patients.
Conclusions: Elderly COPD patients show a varied age-related pattern of disease that warrants specific attention in clinical practice above and beyond assessment of airflow limitation. Trial registration Clinical trial registered with the University Hospital Medical Information Network (UMIN000003470, April 10, 2010).
Figures
References
-
- United Nations Department of Economic and Social Affairs Population Division. World population prospects: the 2010 revision, volume I Comprehensive Tables. 2011. http://esa.un.org/wpp/documentation/pdf/WPP2010_Volume-I_Comprehensive-T.... Accessed 22 July 2015.
-
- Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease. Updated 2015. http://www.goldcopd.org/uploads/users/files/GOLD_Report_2015.pdf. Accessed 22 July 2015.
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
