

Hemodynamic coherence and the rationale for monitoring the microcirculation
- PMID: 26729241
- PMCID: PMC4699073
- DOI: 10.1186/cc14726
Hemodynamic coherence and the rationale for monitoring the microcirculation
Abstract
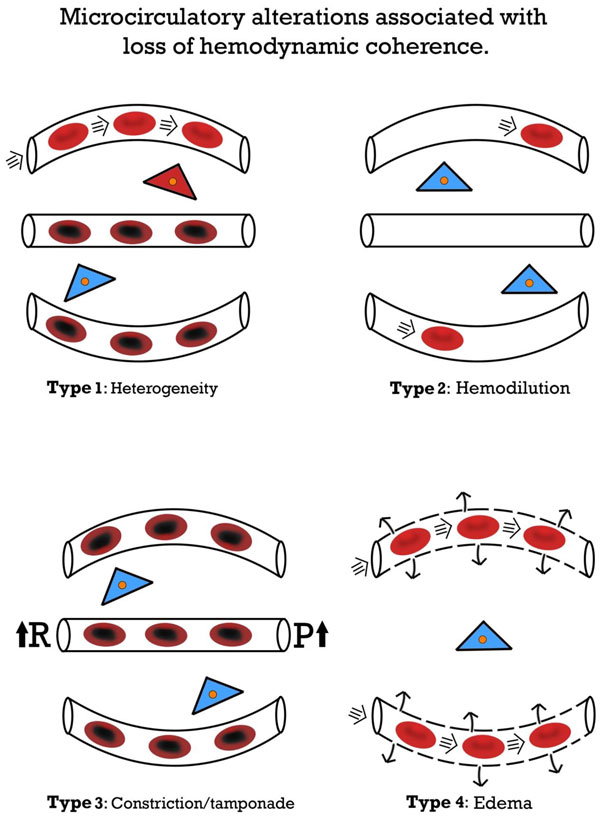
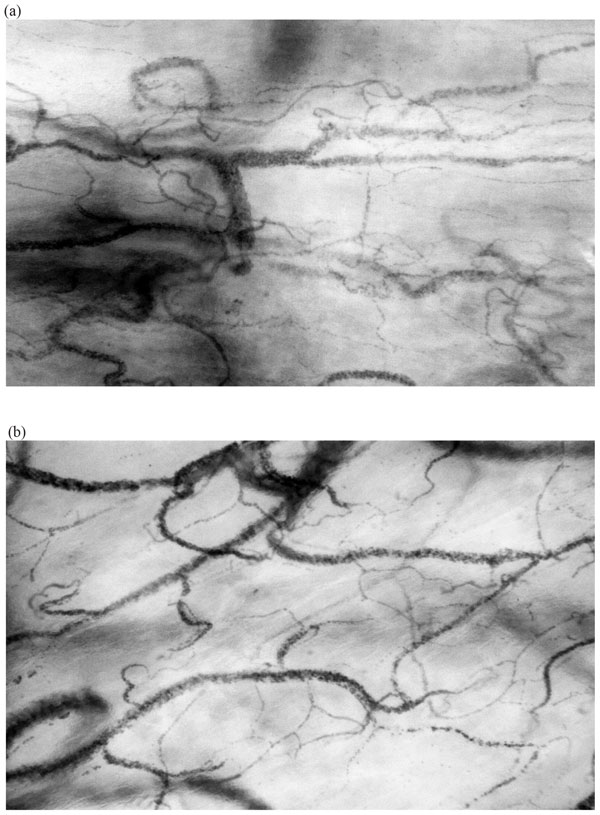
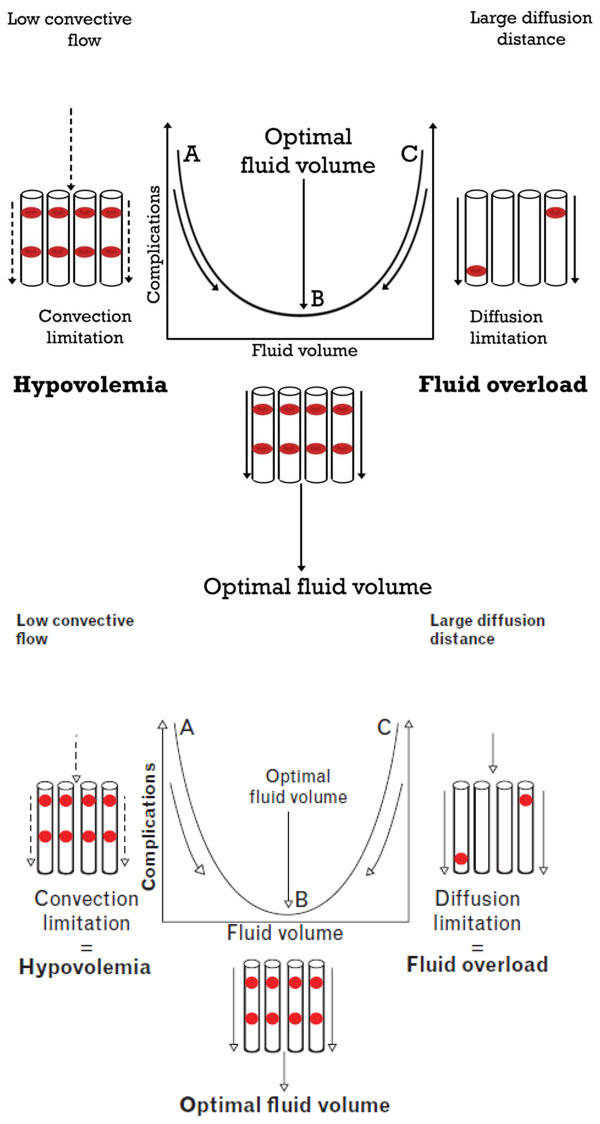
This article presents a personal viewpoint of the shortcoming of conventional hemodynamic resuscitation procedures in achieving organ perfusion and tissue oxygenation following conditions of shock and cardiovascular compromise, and why it is important to monitor the microcirculation in such conditions. The article emphasizes that if resuscitation procedures are based on the correction of systemic variables, there must be coherence between the macrocirculation and microcirculation if systemic hemodynamic-driven resuscitation procedures are to be effective in correcting organ perfusion and oxygenation. However, in conditions of inflammation and infection, which often accompany states of shock, vascular regulation and compensatory mechanisms needed to sustain hemodynamic coherence are lost, and the regional circulation and microcirculation remain in shock. We identify four types of microcirculatory alterations underlying the loss of hemodynamic coherence: type 1, heterogeneous microcirculatory flow; type 2, reduced capillary density induced by hemodilution and anemia; type 3, microcirculatory flow reduction caused by vasoconstriction or tamponade; and type 4, tissue edema. These microcirculatory alterations can be observed at the bedside using direct visualization of the sublingual microcirculation with hand-held vital microscopes. Each of these alterations results in oxygen delivery limitation to the tissue cells despite the presence of normalized systemic hemodynamic variables. Based on these concepts, we propose how to optimize the volume of fluid to maximize the oxygen-carrying capacity of the microcirculation to transport oxygen to the tissues.
Figures
References
-
- Finfer S, Bellomo R, Boyce N, French J, Myburgh J, Norton R. SAFE Study Investigators. A comparison of albumin and saline for fluid resuscitation in the intensive care unit. N Engl J Med. 2004;350:2247–56. - PubMed
-
- Mouncey PR, Osborn TM, Power GS, Harrison DA, Sadique MZ, Grieve RD, Jahan R, Harvey SE, Bell D, Bion JF, Coats TJ, Singer M, Young JD, Rowan KM. ProMISe Trial Investigators. Trial of early, goal-directed resuscitation for septic shock. N Engl J Med. 2015;372:1301–11. - PubMed
-
- Holst LB, Haase N, Wetterslev J, Wernerman J, Guttormsen AB, Karlsson S, Johansson PI, Aneman A, Vang ML, Winding R, Nebrich L, Nibro HL, Rasmussen BS, Lauridsen JR, Nielsen JS, Oldner A, Pettilä V, Cronhjort MB, Andersen LH, Pedersen UG, Reiter N, Wiis J, White JO, Russell L, Thornberg KJ, Hjortrup PB, Müller RG, Møller MH, Steensen M, Tjäder I, Kilsand K, Odeberg-Wernerman S, Sjøbø B, Bundgaard H, Thyø MA, Lodahl D, Mærkedahl R, Albeck C, Illum D, Kruse M, Winkel P, Perner A. TRISS Trial Group; Scandinavian Critical Care Trials Group. Lower versus higher hemoglobin threshold for transfusion in septic shock. N Engl J Med. 2014;371:1381–91. - PubMed
-
- Ranieri VM, Thompson BT, Barie PS, Dhainaut JF, Douglas IS, Finfer S, Gårdlund B, Marshall JC, Rhodes A, Artigas A, Payen D, Tenhunen J, Al-Khalidi HR, Thompson V, Janes J, Macias WL, Vangerow B, Williams MD. PROWESS-SHOCK Study Group. Drotrecogin alfa (activated) in adults with septic shock. N Engl J Med. 2012;366:2055–64. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
