

Importance of Radiation Oncologist Experience Among Patients With Head-and-Neck Cancer Treated With Intensity-Modulated Radiation Therapy
- PMID: 26729432
- PMCID: PMC4872027
- DOI: 10.1200/JCO.2015.63.9898
Importance of Radiation Oncologist Experience Among Patients With Head-and-Neck Cancer Treated With Intensity-Modulated Radiation Therapy
Abstract
Purpose: Over the past decade, intensity-modulated radiation therapy (IMRT) has replaced conventional radiation techniques in the management of head-and-neck cancers (HNCs). We conducted this population-based study to evaluate the influence of radiation oncologist experience on outcomes in patients with HNC treated with IMRT compared with patients with HNC treated with conventional radiation therapy.
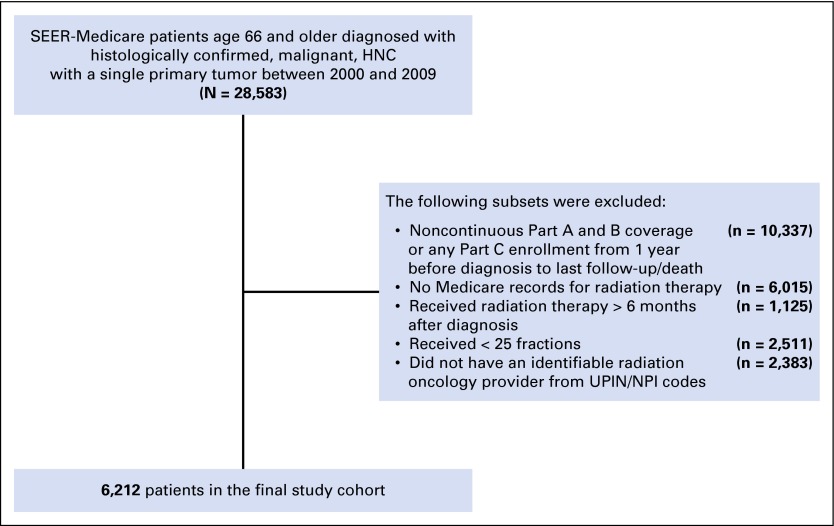
Methods: We identified radiation providers from Medicare claims of 6,212 Medicare beneficiaries with HNC treated between 2000 and 2009. We analyzed the impact of provider volume on all-cause mortality, HNC mortality, and toxicity end points after treatment with either conventional radiation therapy or IMRT. All analyses were performed by using either multivariable Cox proportional hazards or Fine-Gray regression models controlling for potential confounding variables.
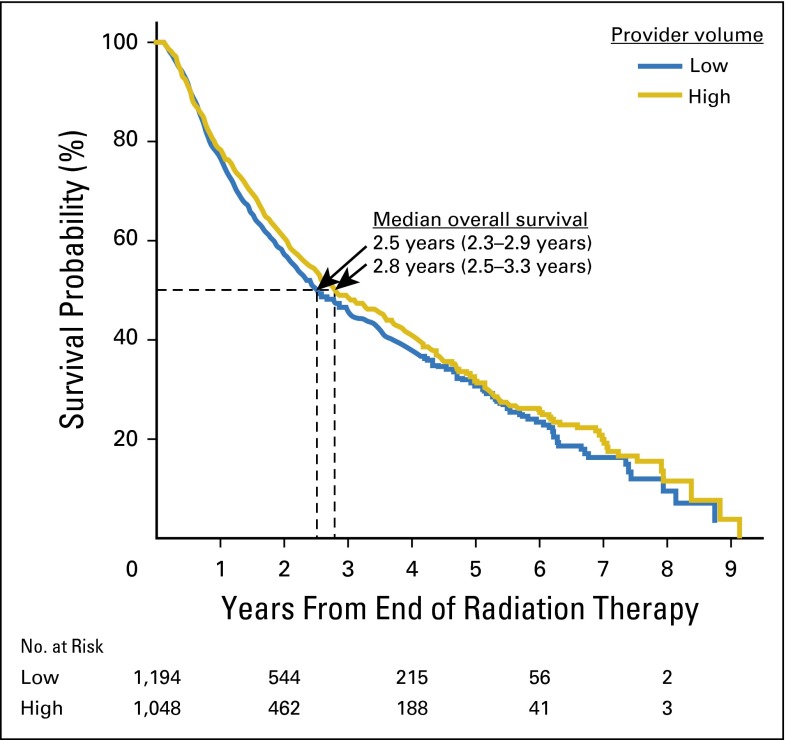
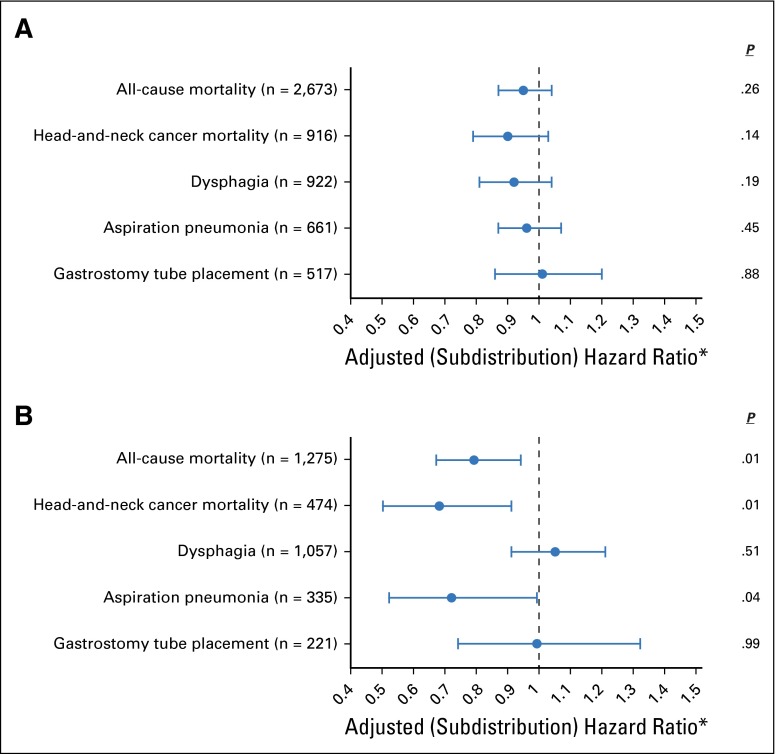
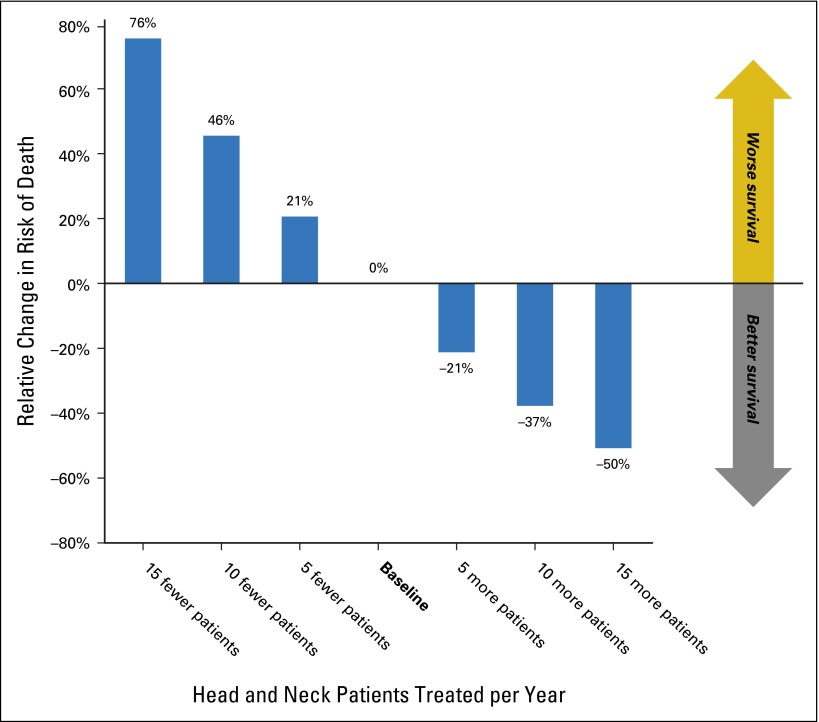
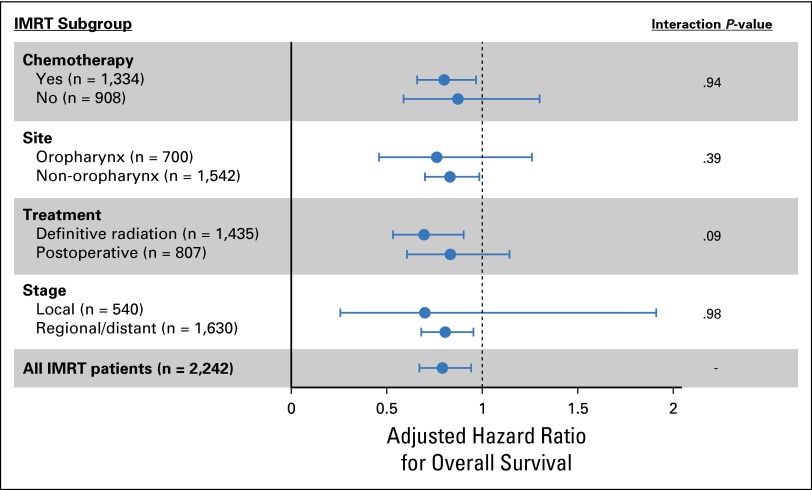
Results: Among patients treated with conventional radiation, we found no significant relationship between provider volume and patient survival or any toxicity end point. Among patients receiving IMRT, those treated by higher-volume radiation oncologists had improved survival compared with those treated by low-volume providers. The risk of all-cause mortality decreased by 21% for every additional five patients treated per provider per year (hazard ratio [HR], 0.79; 95% CI, 0.67 to 0.94). Patients treated with IMRT by higher-volume providers had decreased HNC-specific mortality (subdistribution HR, 0.68; 95% CI, 0.50 to 0.91) and decreased risk of aspiration pneumonia (subdistribution HR, 0.72; 95% CI, 0.52 to 0.99).
Conclusion: Patients receiving IMRT for HNC had improved outcomes when treated by higher-volume providers. These findings will better inform patients and providers when making decisions about treatment, and emphasize the critical importance of high-quality radiation therapy for optimal treatment of HNC.
© 2016 by American Society of Clinical Oncology.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest are found in the article online at
Figures
Comment in
-
Head and Neck Radiation Oncology: Is Busier Better?J Clin Oncol. 2016 Mar 1;34(7):653-4. doi: 10.1200/JCO.2015.65.4343. Epub 2016 Jan 4. J Clin Oncol. 2016. PMID: 26729436 No abstract available.
-
Improving Head and Neck Cancer Outcomes: Technology, Used Wisely.Int J Radiat Oncol Biol Phys. 2016 Nov 1;96(3):489-92. doi: 10.1016/j.ijrobp.2016.04.021. Int J Radiat Oncol Biol Phys. 2016. PMID: 27681744 No abstract available.
References
-
- National Comprehensive Cancer Network NCCN Clinical Practice Guidelines in oncology: Head and neck cancers. http://www.nccn.org/professionals/physician_gls/f_guidelines.asp.
-
- Peters LJ, O’Sullivan B, Giralt J, et al. Critical impact of radiotherapy protocol compliance and quality in the treatment of advanced head and neck cancer: Results from TROG 02.02. J Clin Oncol. 2010;28:2996–3001. - PubMed
-
- Kam MK, Leung SF, Zee B, et al. Prospective randomized study of intensity-modulated radiotherapy on salivary gland function in early-stage nasopharyngeal carcinoma patients. J Clin Oncol. 2007;25:4873–4879. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
