

Twelve-Month Estrogen Levels in Premenopausal Women With Hormone Receptor-Positive Breast Cancer Receiving Adjuvant Triptorelin Plus Exemestane or Tamoxifen in the Suppression of Ovarian Function Trial (SOFT): The SOFT-EST Substudy
- PMID: 26729437
- PMCID: PMC4872316
- DOI: 10.1200/JCO.2015.61.2259
Twelve-Month Estrogen Levels in Premenopausal Women With Hormone Receptor-Positive Breast Cancer Receiving Adjuvant Triptorelin Plus Exemestane or Tamoxifen in the Suppression of Ovarian Function Trial (SOFT): The SOFT-EST Substudy
Abstract
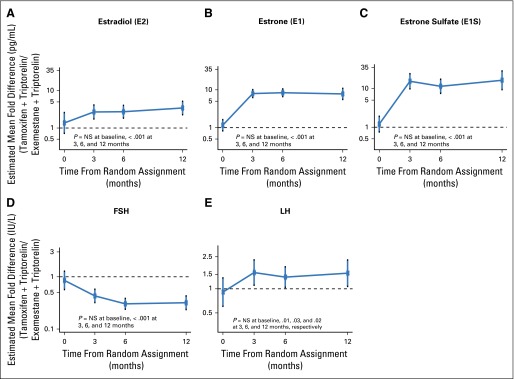
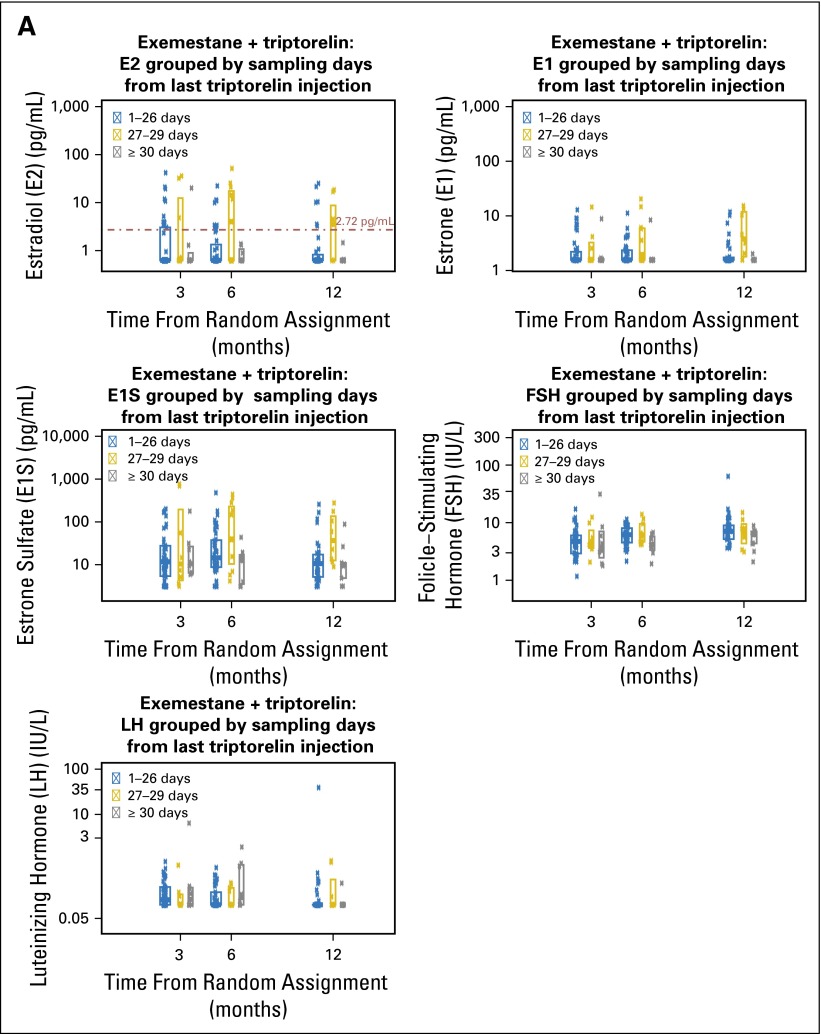
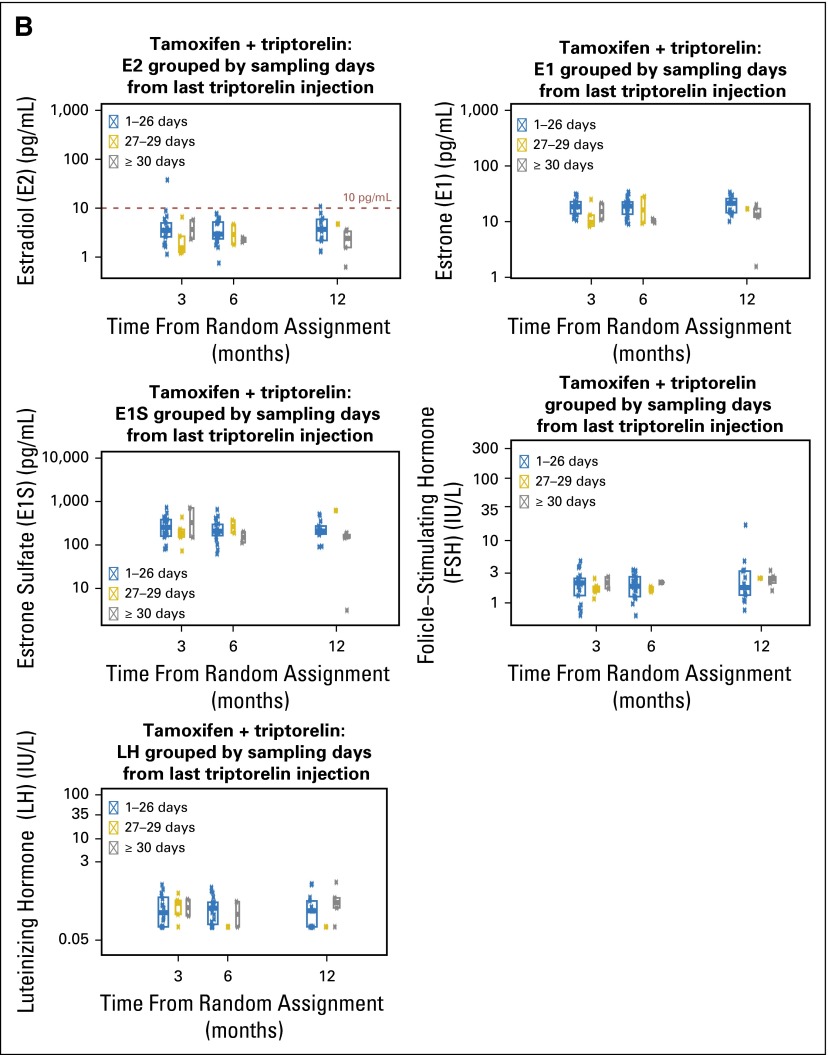
Purpose: To describe estradiol (E2), estrone (E1), and estrone sulfate (E1S) levels during the first year of monthly triptorelin plus exemestane or tamoxifen and to assess possible suboptimal suppression while receiving exemestane plus triptorelin.
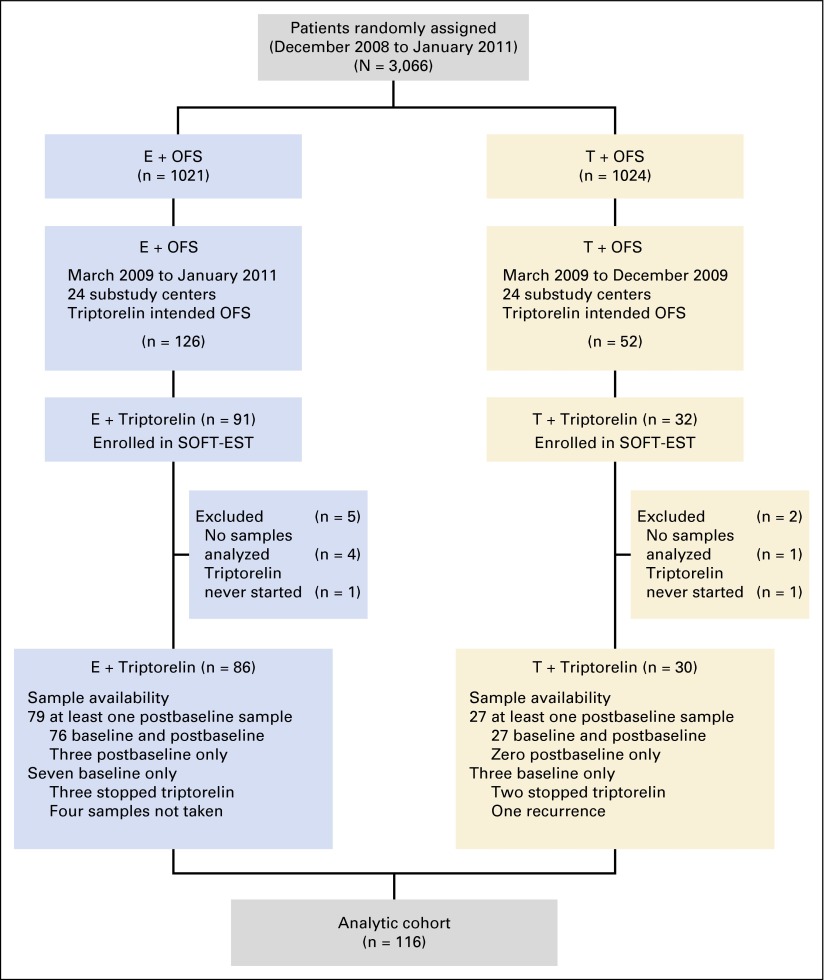
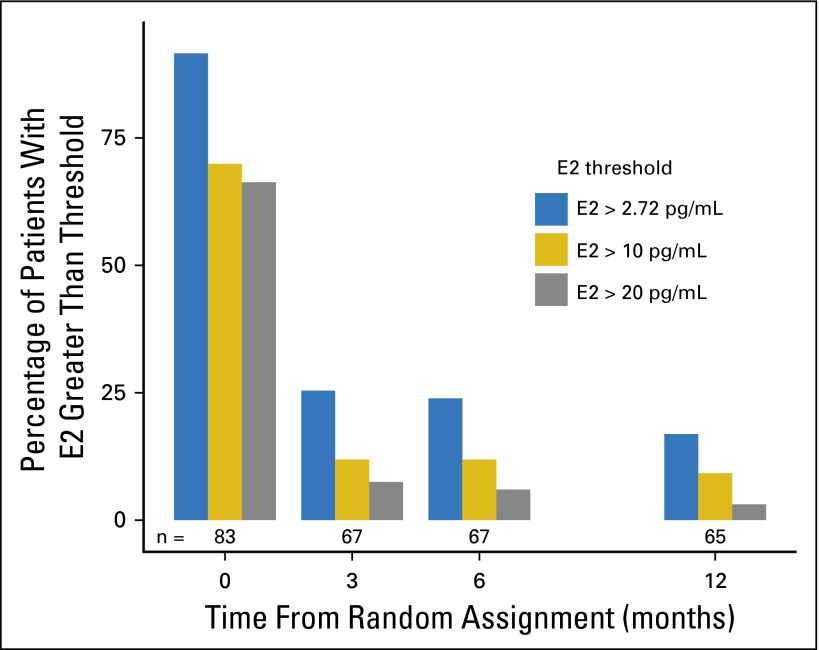
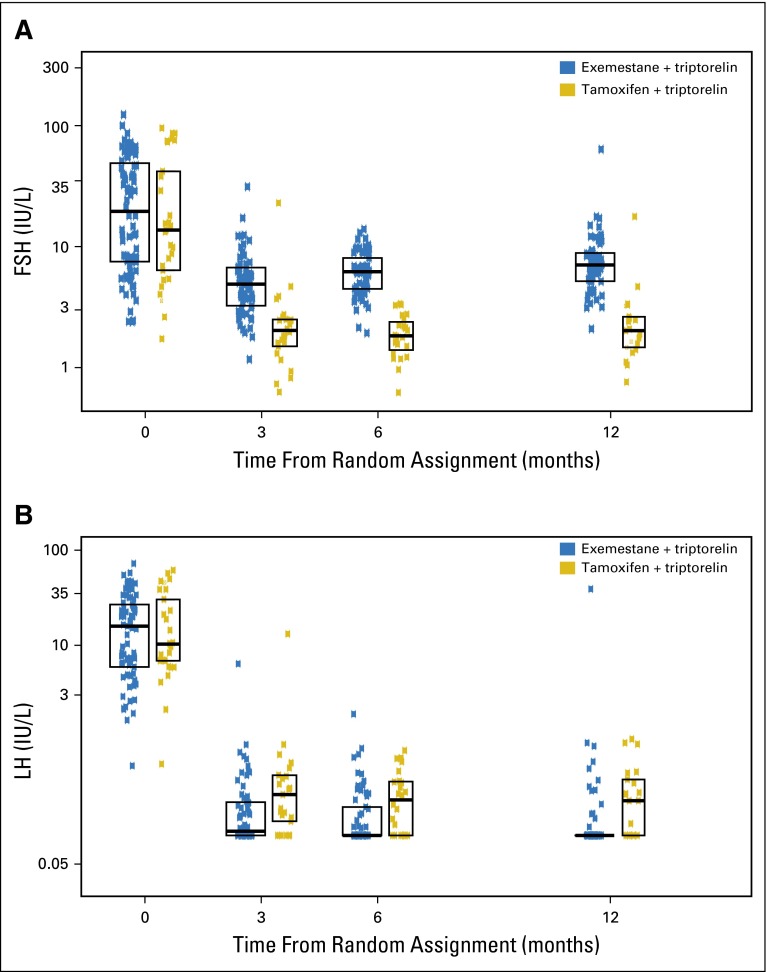
Patients and methods: Premenopausal patients with early breast cancer on the Suppression of Ovarian Function Trial who selected triptorelin as the ovarian suppression method and were randomly assigned to exemestane plus triptorelin or tamoxifen plus triptorelin were enrolled until the target population of 120 patients was reached. Blood sampling time points were 0, 3, 6, 12, 18, 24, 36, and 48 months. Serum estrogens were measured with a highly sensitive and specific assay. This preplanned 12-month analysis evaluated E2, E1, E1S, follicle-stimulating hormone, and luteinizing hormone levels in all patients and the proportion of patients with E2 levels greater than 2.72 pg/mL at any time point during treatment with exemestane plus triptorelin.
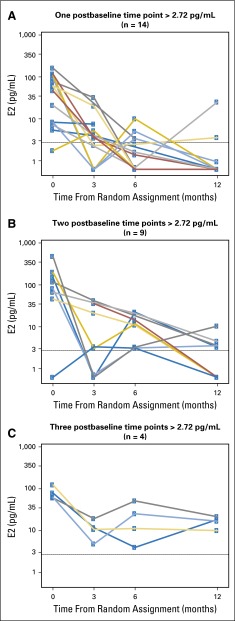
Results: One hundred sixteen patients (exemestane, n = 86; tamoxifen, n = 30; median age, 44 years; median E2, 51 pg/mL; 55% prior chemotherapy) started triptorelin and had one or more samples drawn. With exemestane plus triptorelin, median reductions from baseline E2, E1, and E1S levels were consistently ≥ 95%, resulting in significantly lower levels than with tamoxifen plus triptorelin at all time points. Among patients on exemestane plus triptorelin, 25%, 24%, and 17% had an E2 level greater than 2.72 pg/mL at 3, 6, and 12 months, respectively. Baseline factors related to on-treatment E2 level greater than 2.72 pg/mL were no prior chemotherapy (P = .06), higher body mass index (P = .05), and lower follicle-stimulating hormone and luteinizing hormone (each P < .01).
Conclusion: During the first year, most patients on exemestane plus triptorelin had E2 levels below the defined threshold of 2.72 pg/mL, consistent with levels reported in postmenopausal patients on aromatase inhibitors, but at each time point, at least 17% of patients had levels greater than the threshold.
© 2016 by American Society of Clinical Oncology.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest are found in the article online at
Figures

References
-
- Beatson GW. 1896. On treatment of inoperable cases of carcinoma of the mamma: Suggestions for a new method of treatment, with illustrative cases. Lancet 2:104-107, 162-165,
-
- Boccardo F, Rubagotti A, Perrotta A, et al. Ovarian ablation versus goserelin with or without tamoxifen in pre-perimenopausal patients with advanced breast cancer: Results of a multicentric Italian study. Ann Oncol. 1994;5:337–342. - PubMed
-
- Taylor CW, Green S, Dalton WS, et al. Multicenter randomized clinical trial of goserelin versus surgical ovariectomy in premenopausal patients with receptor-positive metastatic breast cancer: An intergroup study. J Clin Oncol. 1998;16:994–999. - PubMed
-
- Blamey RW, Jonat W, Kaufmann M, et al. Goserelin depot in the treatment of premenopausal advanced breast cancer. Eur J Cancer. 1992;28A:810–814. - PubMed
-
- Schmid P, Untch M, Kossé V, et al. Leuprorelin acetate every-3-months depot versus cyclophosphamide, methotrexate, and fluorouracil as adjuvant treatment in premenopausal patients with node-positive breast cancer: The TABLE study. J Clin Oncol. 2007;25:2509–2515. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
