

Population Pharmacokinetics of Colistin Methanesulfonate and Colistin in Critically Ill Patients with Acute Renal Failure Requiring Intermittent Hemodialysis
- PMID: 26729492
- PMCID: PMC4775947
- DOI: 10.1128/AAC.01868-15
Population Pharmacokinetics of Colistin Methanesulfonate and Colistin in Critically Ill Patients with Acute Renal Failure Requiring Intermittent Hemodialysis
Abstract
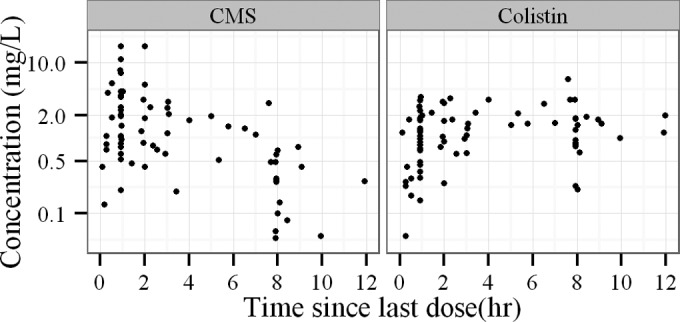
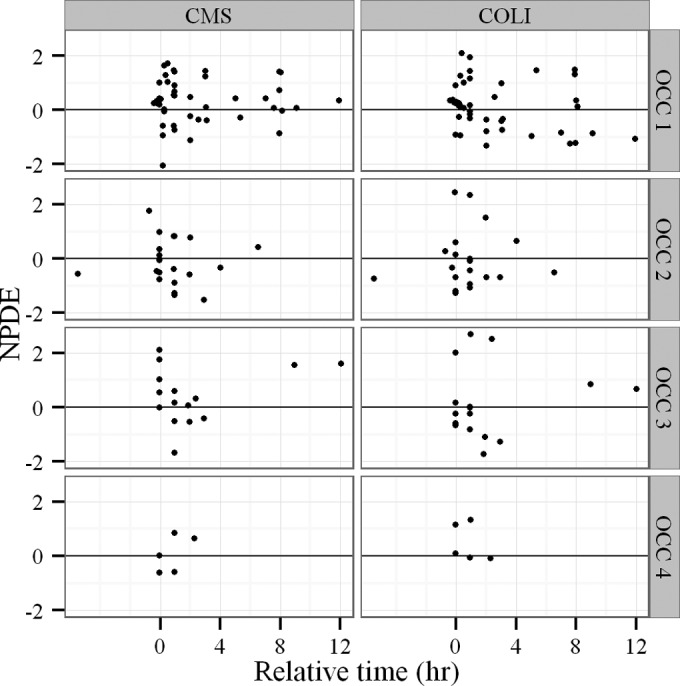
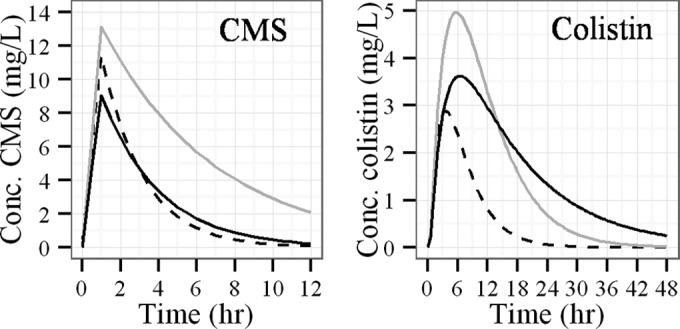
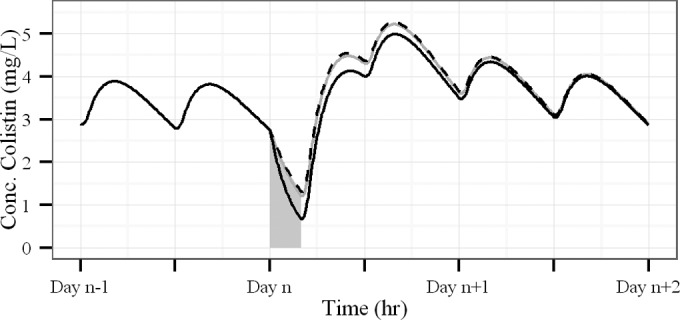
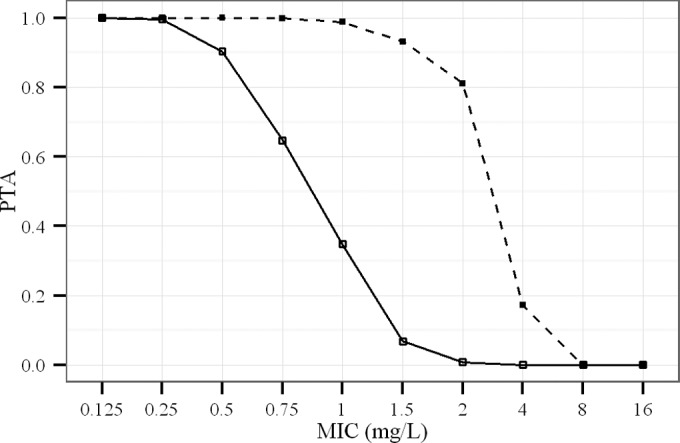
Colistin is increasingly used as a last option for the treatment of severe infections due to Gram-negative bacteria in critically ill patients requiring intermittent hemodialysis (HD) for acute renal failure. Our objective was to characterize the pharmacokinetics (PK) of colistin and its prodrug colistin methanesulfonate (CMS) in this population and to suggest dosing regimen recommendations. Eight intensive care unit (ICU) patients who were under intermittent HD and who were treated by CMS (Colimycine) were included. Blood samples were collected between two consecutive HD sessions. CMS and colistin concentrations were measured by a specific chromatographic assay and were analyzed using a PK population approach (Monolix software). Monte Carlo simulations were conducted to predict the probability of target attainment (PTA). CMS nonrenal clearance was increased in ICU-HD patients. Compared with that of ICU patients included in the same clinical trial but with preserved renal function, colistin exposure was increased by 3-fold in ICU-HD patients. This is probably because a greater fraction of the CMS converted into colistin. To maintain colistin plasma concentrations high enough (>3 mg/liter) for high PTA values (area under the concentration-time curve for the free, unbound fraction of a drug [fAUC]/MIC of >10 and fAUC/MIC of >50 for systemic and lung infections, respectively), at least for MICs lower than 1.5 mg/liter (nonpulmonary infection) or 0.5 mg/liter (pulmonary infection), the dosing regimen of CMS should be 1.5 million international units (MIU) twice daily on non-HD days. HD should be conducted at the end of a dosing interval, and a supplemental dose of 1.5 MIU should be administered after the HD session (i.e., total of 4.5 MIU for HD days). This study has confirmed and complemented previously published data and suggests an a priori clear and easy to follow dosing strategy for CMS in ICU-HD patients.
Copyright © 2016, American Society for Microbiology. All Rights Reserved.
Figures
References
-
- Nation RL, Li J, Cars O, Couet W, Dudley MN, Kaye KS, Mouton JW, Paterson DL, Tam VH, Theuretzbacher U, Tsuji BT, Turnidge JD. 2015. Framework for optimisation of the clinical use of colistin and polymyxin B: the Prato polymyxin consensus. Lancet Infect Dis 15:225–234. doi:10.1016/S1473-3099(14)70850-3. - DOI - PubMed
-
- Garonzik SM, Li J, Thamlikitkul V, Paterson DL, Shoham S, Jacob J, Silveira FP, Forrest A, Nation RL. 2011. Population pharmacokinetics of colistin methanesulfonate and formed colistin in critically ill patients from a multicenter study provide dosing suggestions for various categories of patients. Antimicrob Agents Chemother 55:3284–3294. doi:10.1128/AAC.01733-10. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
