

Microbiological and Clinical Effects of Sitafloxacin and Azithromycin in Periodontitis Patients Receiving Supportive Periodontal Therapy
- PMID: 26729495
- PMCID: PMC4775917
- DOI: 10.1128/AAC.02575-15
Microbiological and Clinical Effects of Sitafloxacin and Azithromycin in Periodontitis Patients Receiving Supportive Periodontal Therapy
Abstract
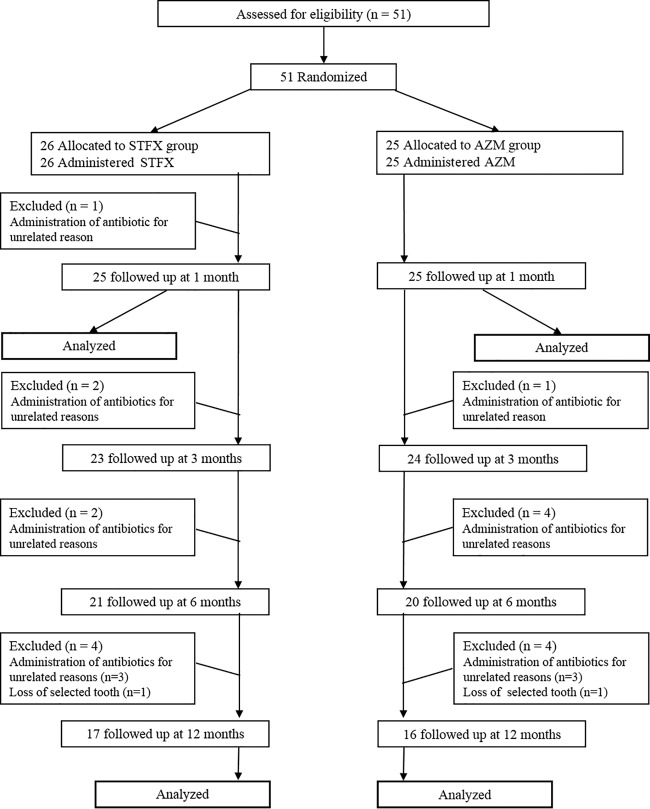
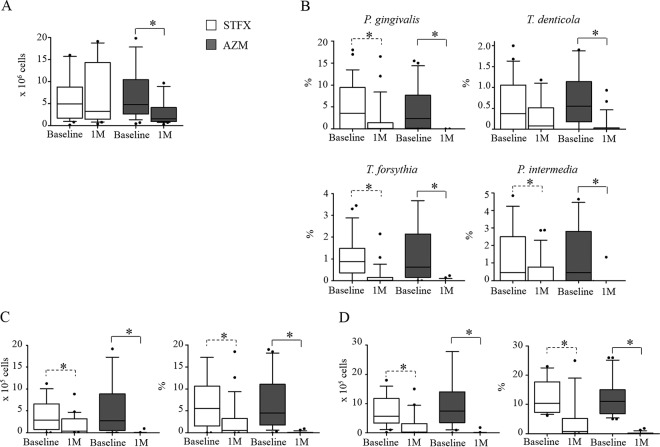
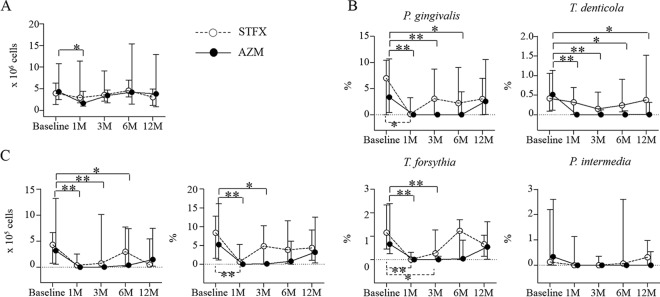
Sitafloxacin (STFX) is a newly developed quinolone that has robust antimicrobial activity against periodontopathic bacteria. We previously reported that oral administration of STFX during supportive periodontal therapy was as effective as conventional mechanical debridement under local anesthesia microbiologically and clinically for 3 months. The aim of the present study was to examine the short-term and long-term microbiological and clinical effects of systemic STFX and azithromycin (AZM) on active periodontal pockets during supportive periodontal therapy. Fifty-one patients receiving supportive periodontal therapy were randomly allocated to the STFX group (200 mg/day of STFX for 5 days) or the AZM group (500 mg/day of AZM for 3 days). The microbiological and clinical parameters were examined until 12 months after the systemic administration of each drug. The concentration of each drug in periodontal pockets and the antimicrobial susceptibility of clinical isolates were also analyzed. The proportions of red complex bacteria, i.e., Porphyromonas gingivalis, Treponema denticola, and Tannerella forsythia, which are the representative periodontopathic bacteria, were significantly reduced at 1 month and remained lower at 12 months than those at baseline in both the STFX and AZM groups. Clinical parameters were significantly improved over the 12-month period in both groups. An increase in the MIC of AZM against clinical isolates was observed in the AZM group. These results indicate that monotherapy with systemic STFX and AZM might be an alternative treatment during supportive periodontal therapy in patients for whom invasive mechanical treatment is inappropriate. (This study has been registered with the University Hospital Medical Information Network-Clinical Trials Registry [UMIN-CTR] under registration number UMIN000007834.).
Copyright © 2016, American Society for Microbiology. All Rights Reserved.
Figures
Similar articles
-
Effects of systemic sitafloxacin on periodontal infection control in elderly patients.Gerodontology. 2012 Jun;29(2):e1024-32. doi: 10.1111/j.1741-2358.2011.00605.x. Epub 2012 Jan 10. Gerodontology. 2012. PMID: 22616908 Clinical Trial.
-
Microbiological effects of periodontal therapy plus azithromycin in patients with diabetes: results from a randomized clinical trial.Acta Odontol Latinoam. 2014;27(2):89-95. doi: 10.1590/S1852-48342014000200008. Acta Odontol Latinoam. 2014. PMID: 25523961 Clinical Trial.
-
Effect of adjunctive systemic azithromycin with periodontal surgery in the treatment of chronic periodontitis in smokers: a pilot study.J Periodontol. 2007 Oct;78(10):1887-96. doi: 10.1902/jop.2007.070072. J Periodontol. 2007. PMID: 17915999 Free PMC article. Clinical Trial.
-
Azithromycin: a new concept in adjuvant treatment of periodontitis.Eur J Pharmacol. 2013 Apr 5;705(1-3):135-9. doi: 10.1016/j.ejphar.2013.02.044. Epub 2013 Mar 13. Eur J Pharmacol. 2013. PMID: 23499686 Review.
-
[Pathogenic potential of Porphyromonas gingivalis, Treponema denticola and Tannerella forsythia, the red bacterial complex associated with periodontitis].Pathol Biol (Paris). 2007 Apr-May;55(3-4):154-62. doi: 10.1016/j.patbio.2006.07.045. Epub 2006 Oct 17. Pathol Biol (Paris). 2007. PMID: 17049750 Review. French.
Cited by
-
Systemic azithromycin as an adjunct to scaling and root planing in patients with stage III/IV periodontitis: 12-month results of a randomized controlled clinical trial.Clin Oral Investig. 2021 Oct;25(10):5997-6006. doi: 10.1007/s00784-021-03906-8. Epub 2021 Mar 30. Clin Oral Investig. 2021. PMID: 33786649 Clinical Trial.
-
Sitafloxacin Expresses Potent Anti-Mycobacterium abscessus Activity.Front Microbiol. 2022 Jan 6;12:779531. doi: 10.3389/fmicb.2021.779531. eCollection 2021. Front Microbiol. 2022. PMID: 35069482 Free PMC article.
-
Construction of a versatile in vitro cultivation screening platform using human oral microbiota.Environ Microbiol Rep. 2024 Apr;16(2):e13243. doi: 10.1111/1758-2229.13243. Environ Microbiol Rep. 2024. PMID: 38425145 Free PMC article.
-
First reported Tannerella forsythia infection in a patient with extensive bronchiectasis: a case report.Front Med (Lausanne). 2025 Apr 28;12:1571506. doi: 10.3389/fmed.2025.1571506. eCollection 2025. Front Med (Lausanne). 2025. PMID: 40357303 Free PMC article.
-
Supportive periodontal therapy (SPT) for maintaining the dentition in adults treated for periodontitis.Cochrane Database Syst Rev. 2018 Jan 1;1(1):CD009376. doi: 10.1002/14651858.CD009376.pub2. Cochrane Database Syst Rev. 2018. PMID: 29291254 Free PMC article.
References
-
- Okui T, Aoki-Nonaka Y, Nakajima T, Yamazaki K. 2014. The role of distinct T cell subsets in periodontitis—studies from humans and rodent models. Curr Oral Health Rep 1:114–123. doi:10.1007/s40496-014-0013-z. - DOI
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
