

Patient outcomes following discharge from secure psychiatric hospitals: systematic review and meta-analysis
- PMID: 26729842
- PMCID: PMC4698562
- DOI: 10.1192/bjp.bp.114.149997
Patient outcomes following discharge from secure psychiatric hospitals: systematic review and meta-analysis
Abstract
Background: Secure hospitals are a high-cost, low-volume service consuming around a fifth of the overall mental health budget in England and Wales.
Aims: A systematic review and meta-analysis of adverse outcomes after discharge along with a comparison with rates in other clinical and forensic groups in order to inform public health and policy.
Method: We searched for primary studies that followed patients discharged from a secure hospital, and reported mortality, readmissions or reconvictions. We determined crude rates for all adverse outcomes.
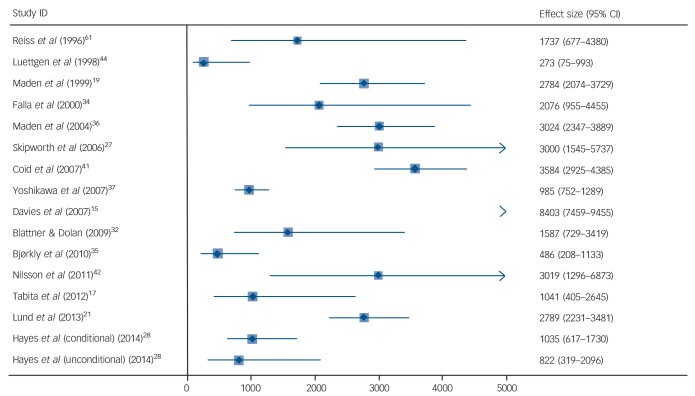
Results: In total, 35 studies from 10 countries were included, involving 12 056 patients out of which 53% were violent offenders. The crude death rate for all-cause mortality was 1538 per 100 000 person-years (95% CI 1175-1901). For suicide, the crude death rate was 325 per 100 000 person-years (95% CI 235-415). The readmission rate was 7208 per 100 000 person-years (95% CI 5916-8500). Crude reoffending rates were 4484 per 100 000 person-years (95% CI 3679-5287), with lower rates in more recent studies.
Conclusions: There is some evidence that patients discharged from forensic psychiatric services have lower offending outcomes than many comparative groups. Services could consider improving interventions aimed at reducing premature mortality, particularly suicide, in discharged patients.
© The Royal College of Psychiatrists 2016.
Conflict of interest statement
None.
Figures




References
-
- Durcan G, Hoare T, Cumming I. Unlocking Pathways to Secure Mental Health Care. Centre for Mental Health, 2011.
-
- Wilson S, James D, Forrester A. The medium-secure project and criminal justice mental health. Lancet 2011; 378: 110–1. - PubMed
-
- Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med 2009; 151: 264–9. - PubMed
-
- Wells G, Shea B, O'Connell D, Peterson J, Welch V, Losos M, et al. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Ottawa Hospital Research Institute, 2000. (http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp) (accessed 26.11.2014).
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
