

Review
doi: 10.1161/CIRCEP.115.003121.
Clinical Spectrum of PRKAG2 Syndrome
Affiliations
- PMID: 26729852
- PMCID: PMC4704128
- DOI: 10.1161/CIRCEP.115.003121
Item in Clipboard
Review
Clinical Spectrum of PRKAG2 Syndrome
Circ Arrhythm Electrophysiol.
2016 Jan.
No abstract available
Keywords: Wolff-Parkinson-White syndrome; atrioventricular block; cardiomyopathy, hypertrophic; death, sudden, cardiac; defibrillators, implantable.
Figures
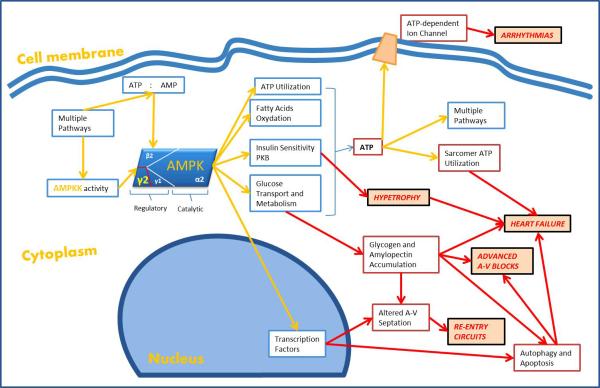
AMPK is activated by high AMP (adenosine monophosphate) levels and by AMPK-kinase. It acts by enhancing glucose and lipids metabolism in order to elevate intracellular ATP. The enzyme also regulates the creatine kinase activity to reduce the ATP depletion. AMPK is also implicated in cardiac development, growth, and regeneration acting through PKB activation and insulin sensitivity. The dysfunction of the enzyme caused by mutations in its γ2 regulatory subunit can cause alterations in numerous secondary pathways and to the unregulated activation of nuclear transcriptional factors. All these effects can lead to cardiac hypertrophy, improper glycogen accumulation, ion channel dysfunctions, altered atrio-ventricular (AV) septation and ATP utilization by sarcomere, which seem to be the substrates for the various clinical features of PRKAG2 syndrome. PKB: protein kinase B; Red arrows: pathological pathway; Yellow arrows: normal pathway.
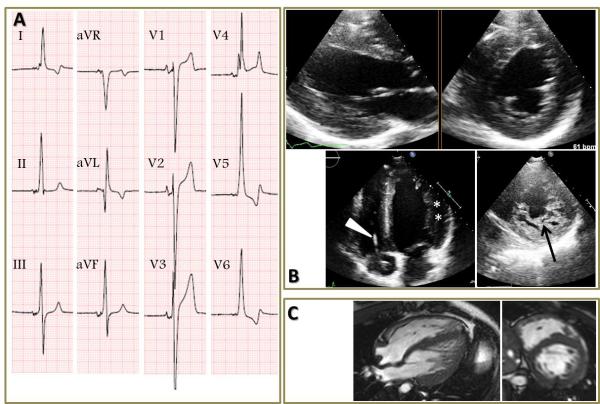
Panel A. Electrocardiogram of a patient with PRKAG2 syndrome, showing a short PR with a delta wave (negative in aVL, positive in I and inferior leads), very high voltages in the QRS complexes, which appear fragmented in V4. Panel B. Transthoracic echocardiogram of the same patient, showing only mildly increased wall thickness of the lateral wall (14mm, asterisks). A pacemaker lead (triangle) is visible in the right side of the heart. Short axis image of the left ventricular apex demonstrates evident trabecules (arrow). Panel C. Cardiovascular magnetic resonance of the same patient (cine images) confirming the echocardiogram findings. T2 weighted images and T1 weighted images post contrast were unremarkable (not shown).
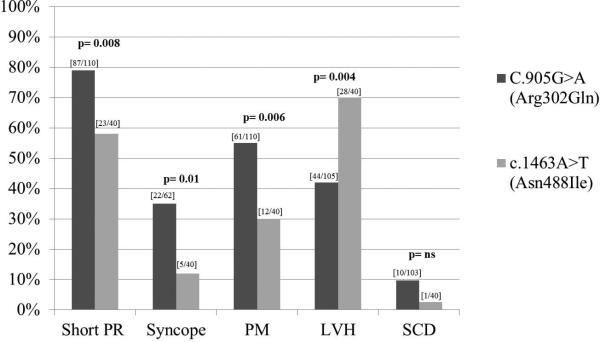
Bar chart comparing the main clinical features between the recurrent Arg302Gln and Asn488Ile mutations. LVH: left ventricular hypertrophy; ns: not statistically significant; PM: pacemaker (implantation); SCD: sudden cardiac death; square brackets: patients with clinical feature/tot number of patients with available data. Statistical analysis was obtained using Fisher's exact test for the “sudden cardiac death” variable; for the other variables, Chi-square test was used.
References
-
- Lev M, Leffler WB, Langendorf R, Pick A. Anatomic findings in a case of ventricular pre-excitation (WPW) terminating in complete atrioventricular block. Circulation. 1966;34:718–733. - PubMed
-
- Gulotta SJ, Gupta RD, Padmanabhan VT, Morrison J. Familial occurrence of sinus bradycardia, short PR interval, intraventricular conduction defects, recurrent supraventricular tachycardia, and cardiomegaly. Am Heart J. 1977;93:19–29. - PubMed
-
- Khair GZ, Soni JS, Bamrah VS. Syncope in hypertrophic cardiomyopathy. II. Coexistence of atrioventricular block and wolff-parkinson-white syndrome. Am Heart J. 1985;110:1083–1086. - PubMed
-
- Gollob MH, Green MS, Tang AS, Gollob T, Karibe A, Ali Hassan AS, Ahmad F, Lozado R, Shah G, Fananapazir L, Bachinski LL, Roberts R. Identification of a gene responsible for familial wolff-parkinson-white syndrome. N Engl J Med. 2001;344:1823–1831. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
