

Global myocardial strain assessment by different imaging modalities to predict outcomes after ST-elevation myocardial infarction: A systematic review
- PMID: 26730301
- PMCID: PMC4691822
- DOI: 10.4330/wjc.v7.i12.948
Global myocardial strain assessment by different imaging modalities to predict outcomes after ST-elevation myocardial infarction: A systematic review
Abstract
Aim: To conduct a systematic review relating myocardial strain assessed by different imaging modalities for prognostication following ST-elevation myocardial infarction (STEMI).
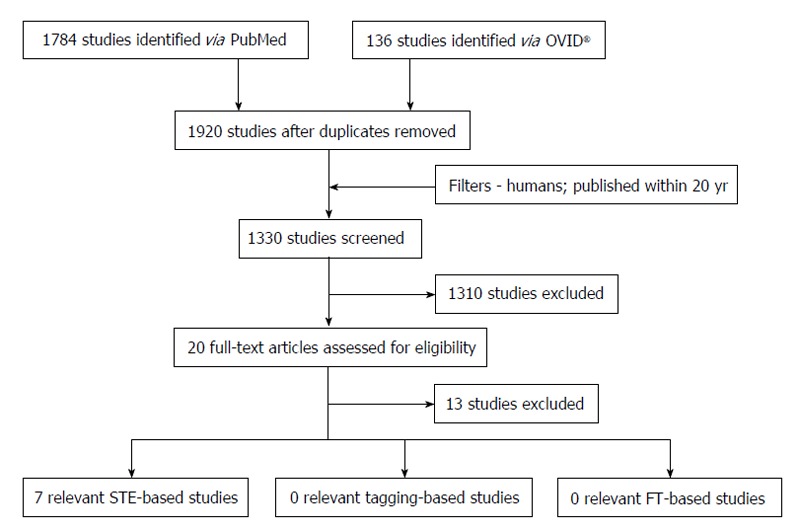
Methods: An online literature search was performed in PubMed and OVID(®) electronic databases to identify any studies that assessed global myocardial strain parameters using speckle-tracking echocardiography (STE) and/or cardiac magnetic resonance imaging (CMR) techniques [either myocardial tagging or feature tracking (FT) software] in an acute STEMI cohort (days 0-14 post-event) to predict prognosis [either development of major adverse cardiac events (MACE)] or adverse left ventricular (LV) remodelling at follow-up (≥ 6 mo for MACE, ≥ 3 mo for remodelling). Search was restricted to studies within the last 20 years. All studies that matched the pre-defined search criteria were reviewed and their results interpreted. Due to considerable heterogeneity between studies, meta-analysis was not performed.
Results: A total of seven studies (n = 7) were identified that matched the search criteria. All studies used STE to evaluate strain parameters - five (n = 5) assessed global longitudinal strain (GLS) (n = 5), one assessed GLS rate (GLS-R) (n = 1) and one assessed both (n = 1). Three studies showed that GLS independently predicted the development of adverse LV remodelling by multivariate analysis - odds ratio between 1.19 (CI: 1.04-1.37, P < 0.05) and 10 (CI: 6.7-14, P < 0.001) depending on the study. Four studies showed that GLS predicted the development of MACE - hazard ratio (HR) between 1.1 (CI: 1-1.1, P = 0.006) and 2.34 (1.10-4.97, P < 0.05). One paper found that GLS-R could significantly predict MACE - HR 18 (10-35, P < 0.001) - whilst another showed it did not. GLS < -10.85% had sensitivity/specificity of 89.7%/91% respectively for predicting the development of remodelling whilst GLS < -13% could predict the development of MACE with sensitivity/specificity of 100%/89% respectively. No suitable studies were identified that assessed global strain by CMR tagging or FT techniques.
Conclusion: GLS measured acutely post-STEMI by STE is a predictor of poor prognosis. Further research is needed to show that this is true for CMR-based techniques.
Keywords: Feature tracking; Major adverse cardiac events; Myocardial infarction; Remodelling; Speckle tracking; Strain; Tagging.
Figures
References
-
- Lozano R, Naghavi M, Foreman K, Lim S, Shibuya K, Aboyans V, Abraham J, Adair T, Aggarwal R, Ahn SY, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380:2095–2128. - PMC - PubMed
-
- Kumar P, Clark M. Acute Coronary Syndromes - Cardiovascular Disease. Kumar and Clark’s Clinical Medicine. 8th ed. Elsevier: 2012. pp. 733–740.
-
- Steg PG, James SK, Atar D, Badano LP, Blömstrom-Lundqvist C, Borger MA, Di Mario C, Dickstein K, Ducrocq G, Fernandez-Aviles F, et al. ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. Eur Heart J. 2012;33:2569–2619. - PubMed
-
- Wilansky S, Moreno CA, Lester SJ. Complications of myocardial infarction. Crit Care Med. 2007;35:S348–S354. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
