

Patient and hospital determinants of primary percutaneous coronary intervention in England, 2003-2013
- PMID: 26732182
- PMCID: PMC4752647
- DOI: 10.1136/heartjnl-2015-308616
Patient and hospital determinants of primary percutaneous coronary intervention in England, 2003-2013
Abstract
Objective: Primary percutaneous coronary intervention (PPCI) for ST-elevation myocardial infarction (STEMI) is insufficiently implemented in many countries. We investigated patient and hospital characteristics associated with PPCI utilisation.
Methods: Whole country registry data (MINAP, Myocardial Ischaemia National Audit Project) comprising PPCI-capable National Health Service trusts in England (84 hospital trusts; 92 350 hospitalisations; 90 489 patients), 2003-2013. Multilevel Poisson regression modelled the relationship between incidence rate ratios (IRR) of PPCI and patient and trust-level factors.
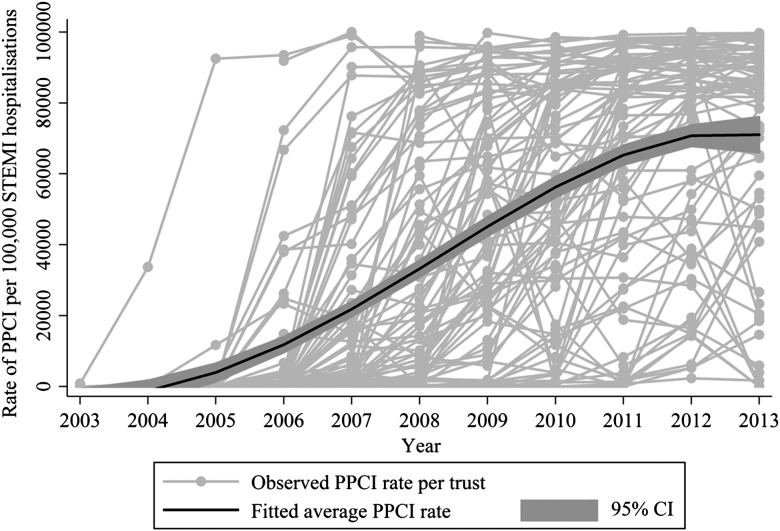
Results: Overall, standardised rates of PPCI increased from 0.01% to 86.3% (2003-2013). While, on average, there was a yearly increase in PPCI utilisation of 30% (adjusted IRR 1.30, 95% CI 1.23 to 1.36), it varied substantially between trusts. PPCI rates were lower for patients with previous myocardial infarction (0.95, 0.93 to 0.98), heart failure (0.86, 0.81 to 0.92), angina (0.96, 0.94 to 0.98), diabetes (0.97, 0.95 to 0.99), chronic renal failure (0.89, 0.85 to 0.90), cerebrovascular disease (0.96, 0.93 to 0.99), age >80 years (0.87, 0.85 to 0.90), and travel distances >30 km (0.95, 0.93 to 0.98). PPCI rates were higher for patients with previous percutaneous coronary intervention (1.09, 1.05 to 1.12) and among trusts with >5 interventional cardiologists (1.30, 1.25 to 1.34), more visiting interventional cardiologists (1-5: 1.31, 1.26 to 1.36; ≥6: 1.42, 1.35 to 1.49), and a 24 h, 7-days-a-week PPCI service (2.69, 2.58 to 2.81). Half of the unexplained variation in PPCI rates was due to between-trust differences.
Conclusions: Following an 8 year implementation phase, PPCI utilisation rates stabilised at 85%. However, older and sicker patients were less likely to receive PPCI and there remained between-trust variation in PPCI rates not attributable to differences in staffing levels. Compliance with clinical pathways for STEMI is needed to ensure more equitable quality of care.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/
Figures

Comment in
-
Variation in primary PCI in England.Heart. 2016 Feb 15;102(4):262. doi: 10.1136/heartjnl-2015-309094. Epub 2016 Jan 5. Heart. 2016. PMID: 26732183 No abstract available.
References
-
- World Health Organization. Tracking University Health Coverage: First Global Monitoring Report. France: WHO, 2015. http://apps.who.int/iris/bitstream/10665/174536/1/9789241564977_eng.pdf?... (accessed 29 Jul 2015).
-
- O'Gara PT, Kushner FG, Ascheim DD, et al. . ACCF/AHA guideline for the management of ST-elevation myocardial infarction: executive summary: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines: developed in collaboration with the American College of Emergency Physicians and Society for Cardiovascular Angiography and Interventions. Catheter Cardiovasc Interv 2013;82:E1–27. 10.1002/ccd.24776 - DOI - PubMed
-
- de Boer SP, Barnes EH, Westerhout CM, et al. . High-risk patients with ST-elevation myocardial infarction derive greatest absolute benefit from primary percutaneous coronary intervention: results from the Primary Coronary Angioplasty Trialist versus thrombolysis (PCAT)-2 collaboration. Am Heart J 2011;161:500–7.e1. 10.1016/j.ahj.2010.11.022 - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources