

Prospective clinical and serological follow-up in early childhood reveals a high rate of subclinical RSV infection and a relatively high reinfection rate within the first 3 years of life
- PMID: 26732801
- PMCID: PMC9150639
- DOI: 10.1017/S0950268815003143
Prospective clinical and serological follow-up in early childhood reveals a high rate of subclinical RSV infection and a relatively high reinfection rate within the first 3 years of life
Abstract
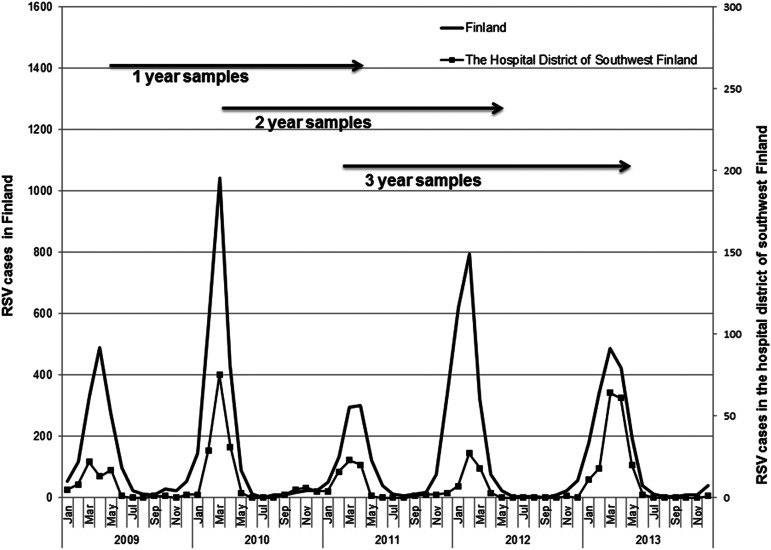
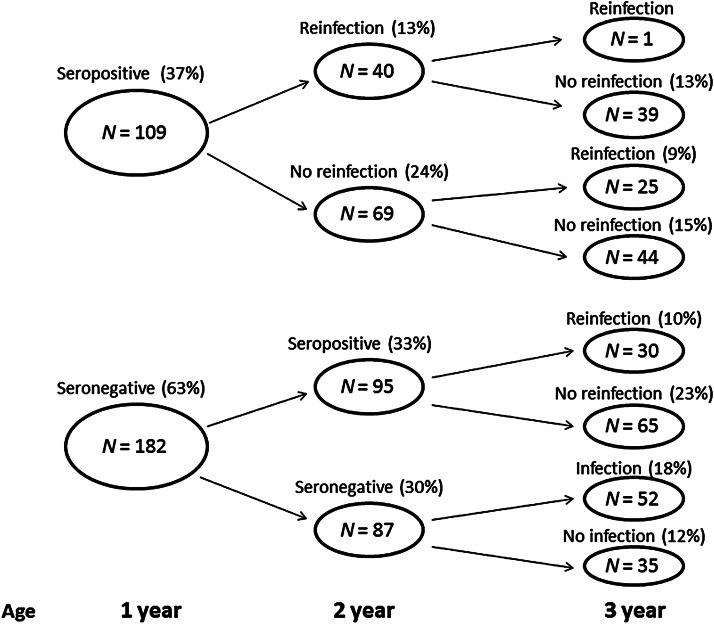
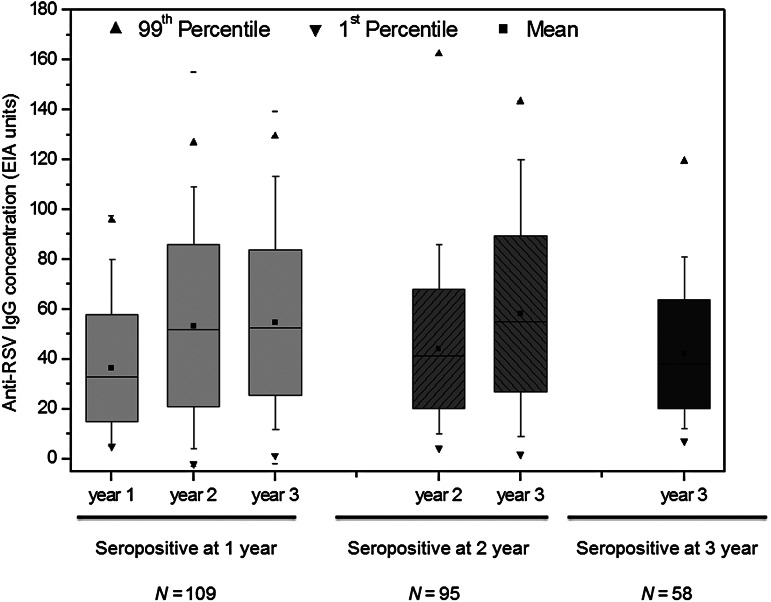
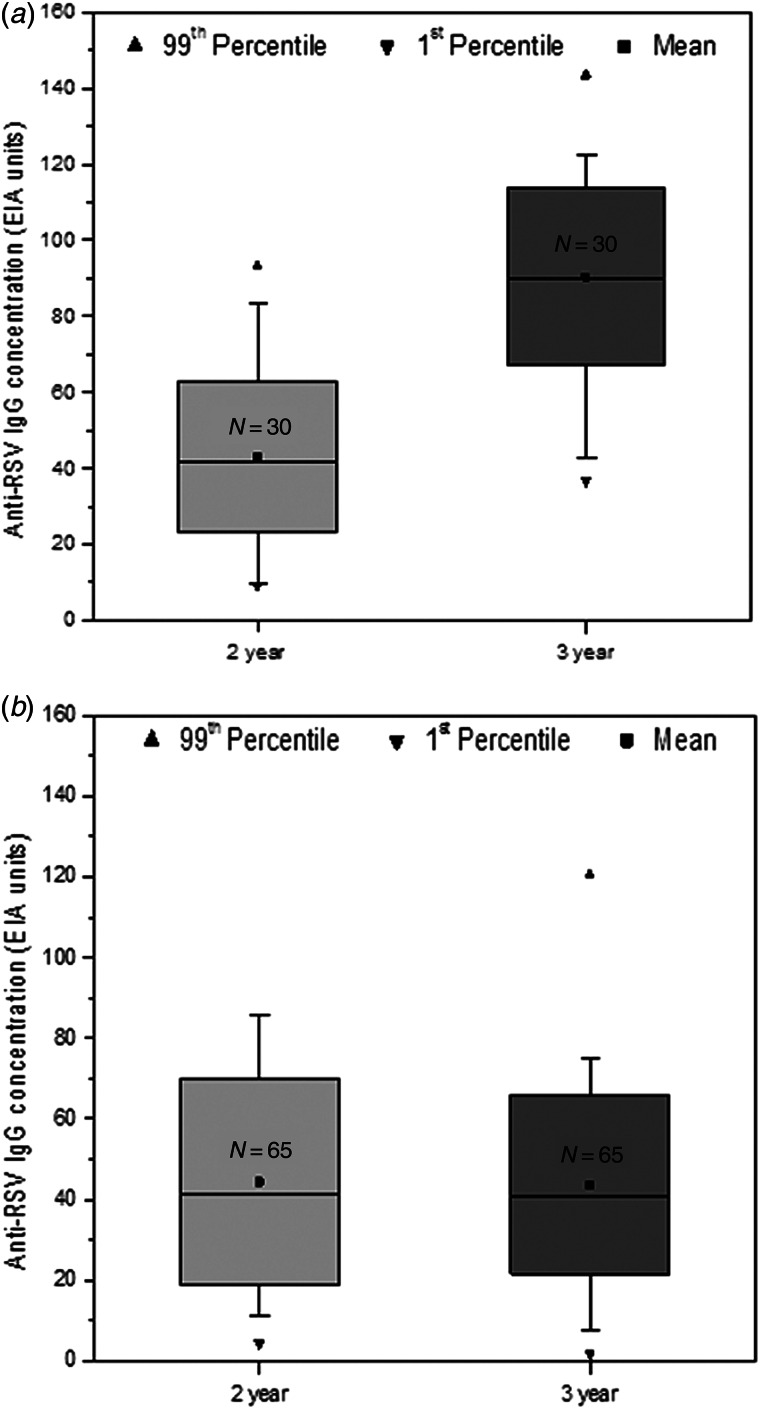
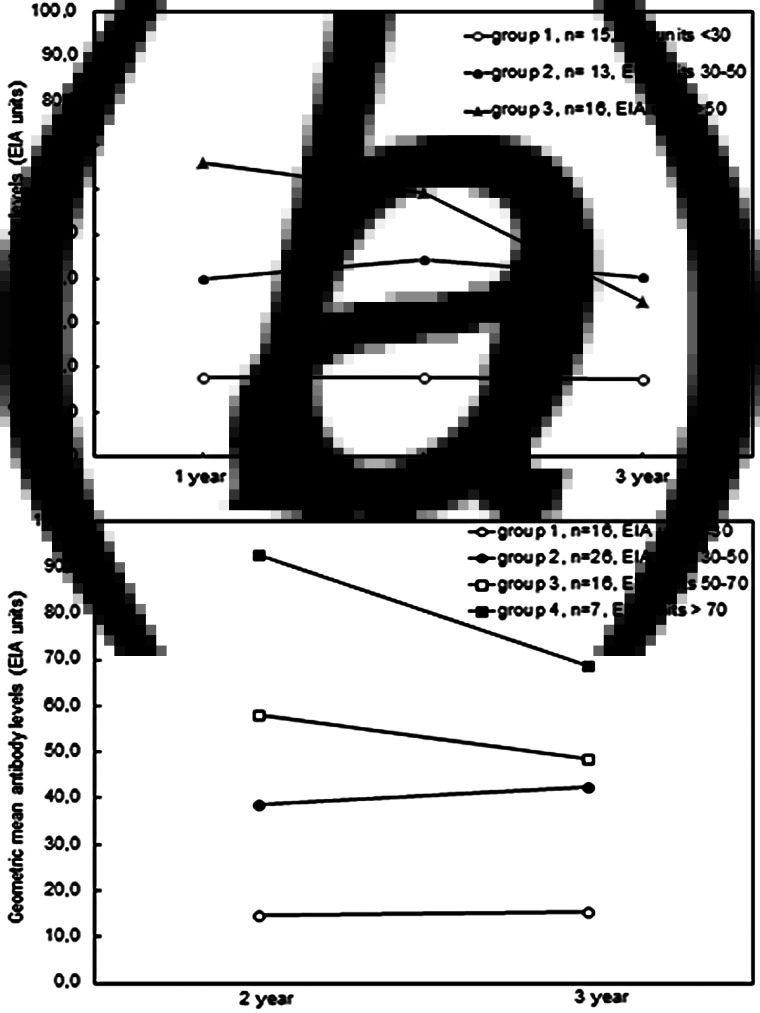
Children encounter repeated respiratory tract infections during their early life. We conducted a prospective clinical and serological follow-up study to estimate the respiratory syncytial virus (RSV) primary infection and reinfection rates in early childhood. Sera were collected from 291 healthy children at the ages of 13, 24 and 36 months and antibody levels against RSV antigens were determined by enzyme immunoassay. The RT-PCR method was also used for identifying the possible presence of RSV in symptomatic patients. At ages 1, 2 and 3 years, 37%, 68% and 86%, respectively, of studied children were seropositive for RSV. In children seropositive at age 1 year, RSV reinfection rate was at least 37%. Only one of reinfected children showed evidence for a third reinfection by age 3 years. Of children who turned RSV seropositive between ages 1 and 2 years, the reinfection rate was 32% during the third year of life. The mean antibody levels at primary infection were very similar in all age groups. The average decrease of antibody levels was 25-30% within a year. In 66 cases RSV infection was identified by RT-PCR. RSV infection rate in early childhood is 86% and reinfection rate is around 35%. This prospective serological follow-up study also provided evidence for the presence of RSV infections in children that did not show clinical signs warranting RSV RNA detection.
Keywords: Antibodies; RSV; infants; reinfection; seroprevalence.
Figures

References
-
- Glezen WP, et al. Risk of primary infection and reinfection with respiratory syncytial virus. American Journal of Diseases of Children 1986; 140: 543–546. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
