

A Distributed Network for Intensive Longitudinal Monitoring in Metastatic Triple-Negative Breast Cancer
- PMID: 26733551
- PMCID: PMC4970582
- DOI: 10.6004/jnccn.2016.0003
A Distributed Network for Intensive Longitudinal Monitoring in Metastatic Triple-Negative Breast Cancer
Abstract
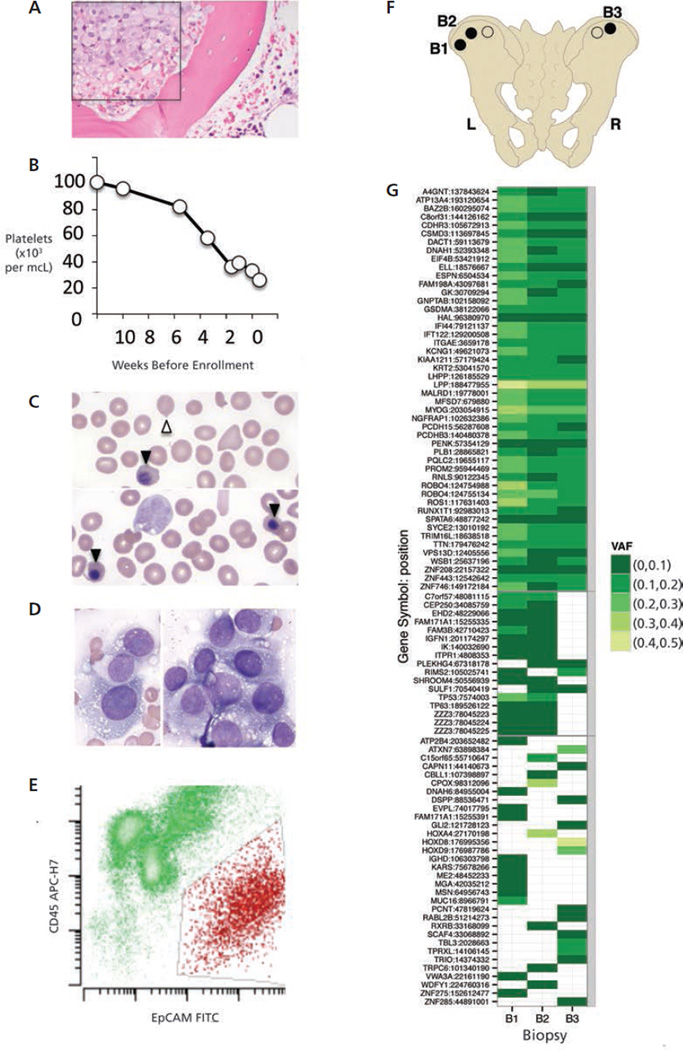
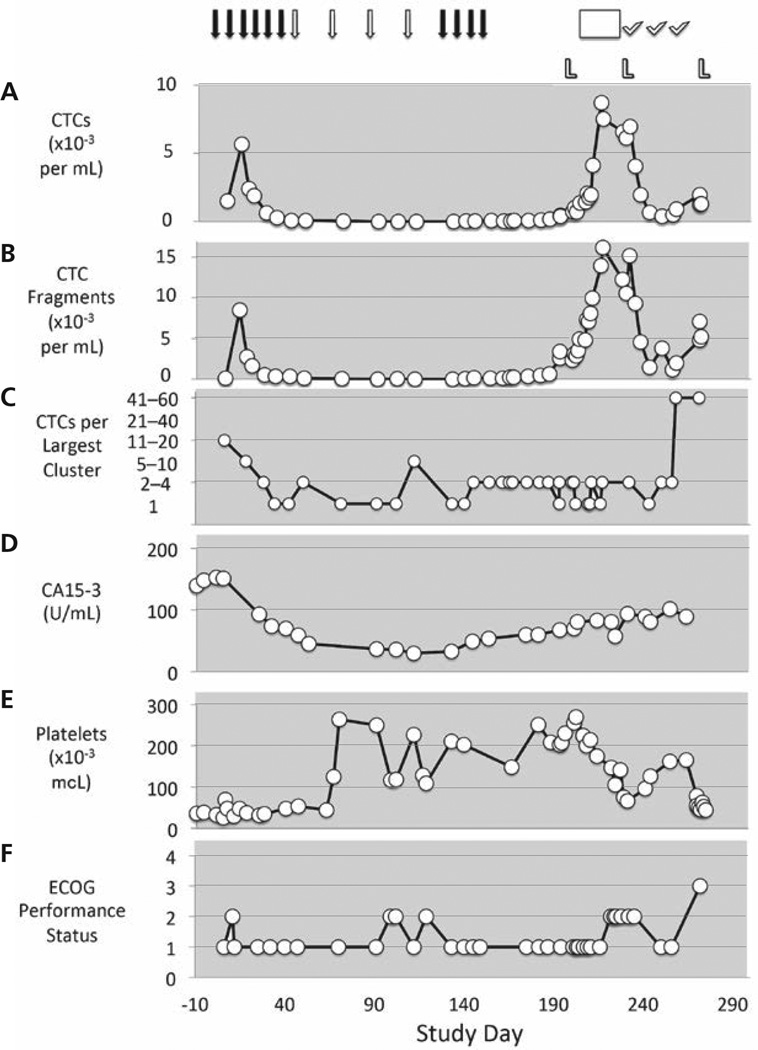
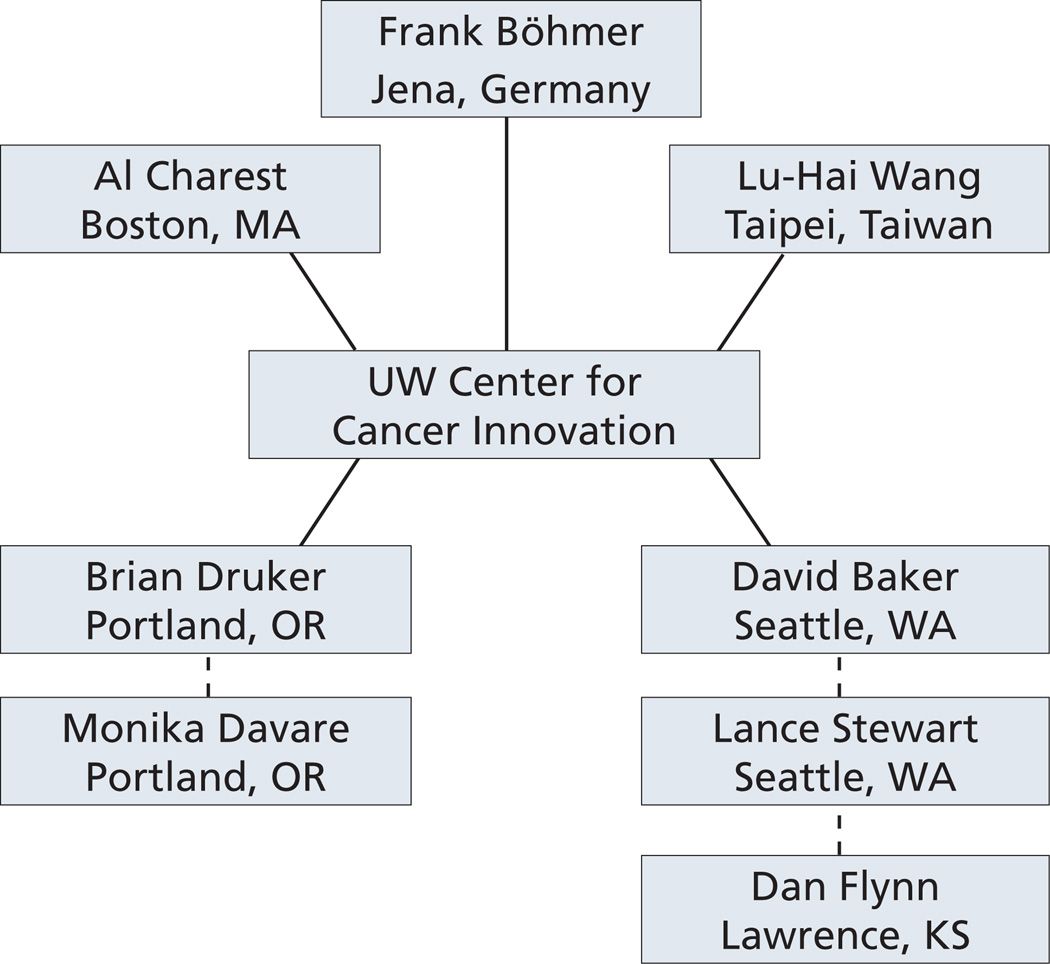
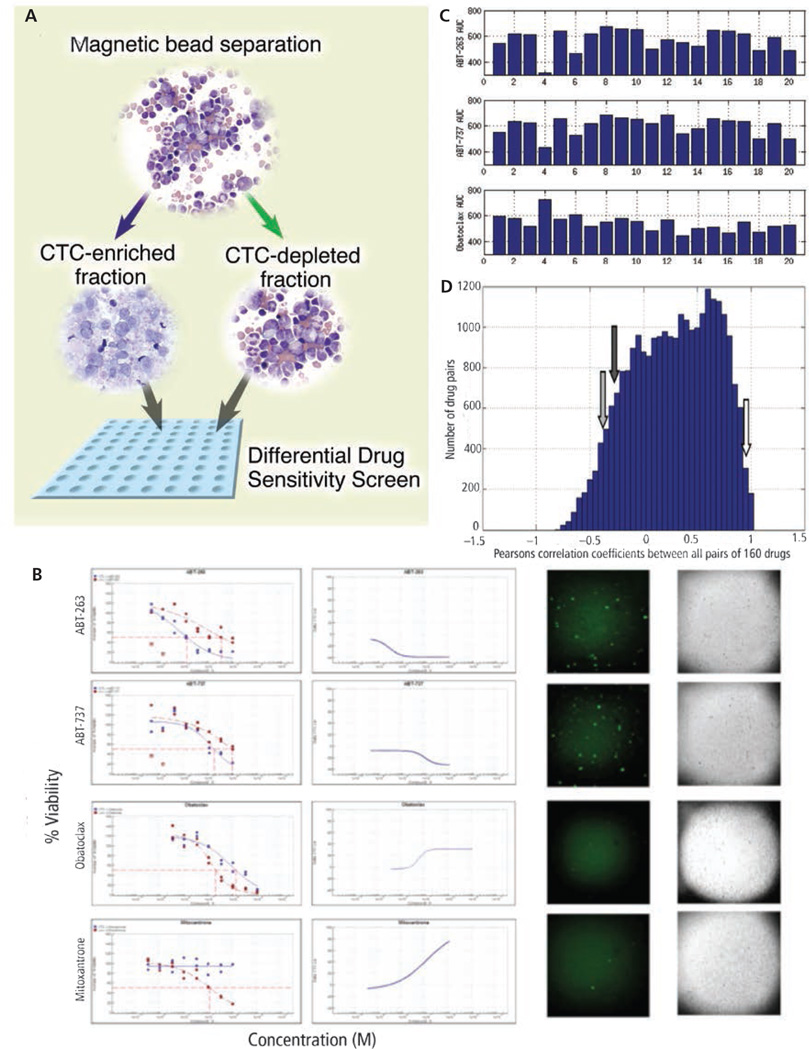
Accelerating cancer research is expected to require new types of clinical trials. This report describes the Intensive Trial of OMics in Cancer (ITOMIC) and a participant with triple-negative breast cancer metastatic to bone, who had markedly elevated circulating tumor cells (CTCs) that were monitored 48 times over 9 months. A total of 32 researchers from 14 institutions were engaged in the patient's evaluation; 20 researchers had no prior involvement in patient care and 18 were recruited specifically for this patient. Whole-exome sequencing of 3 bone marrow samples demonstrated a novel ROS1 variant that was estimated to be present in most or all tumor cells. After an initial response to cisplatin, a hypothesis of crizotinib sensitivity was disproven. Leukapheresis followed by partial CTC enrichment allowed for the development of a differential high-throughput drug screen and demonstrated sensitivity to investigational BH3-mimetic inhibitors of BCL-2 that could not be tested in the patient because requests to the pharmaceutical sponsors were denied. The number and size of CTC clusters correlated with clinical status and eventually death. Focusing the expertise of a distributed network of investigators on an intensively monitored patient with cancer can generate high-resolution views of the natural history of cancer and suggest new opportunities for therapy. Optimization requires access to investigational drugs.
Copyright © 2016 by the National Comprehensive Cancer Network.
Figures

References
-
- Scannell JW, Blanckley A, Boldon H, Warrington B. Diagnosing the decline in pharmaceutical R&D efficiency. Nat Rev Drug Discov. 2012;11:191–200. - PubMed
-
- Nowell PC. The clonal evolution of tumor cell populations. Science. 1976;194:23–28. - PubMed
-
- Dexter DL, Kowalski HM, Blazar BA, et al. Heterogeneity of tumor cells from a single mouse mammary tumor. Cancer Res. 1978;38:3174–3181. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
