

Prevalence and Safety of Off-Label Use of Chemotherapeutic Agents in Older Patients With Breast Cancer: Estimates From SEER-Medicare Data
- PMID: 26733555
- PMCID: PMC4827612
- DOI: 10.6004/jnccn.2016.0007
Prevalence and Safety of Off-Label Use of Chemotherapeutic Agents in Older Patients With Breast Cancer: Estimates From SEER-Medicare Data
Abstract
Background: Prescribing drugs outside of the label indication is legal and may reflect standard practice; however, some off-label use may be inappropriate. This study measured the prevalence and safety of off-label use both in accordance with practice guidelines and inconsistent with practice guidelines in older patients with breast cancer.
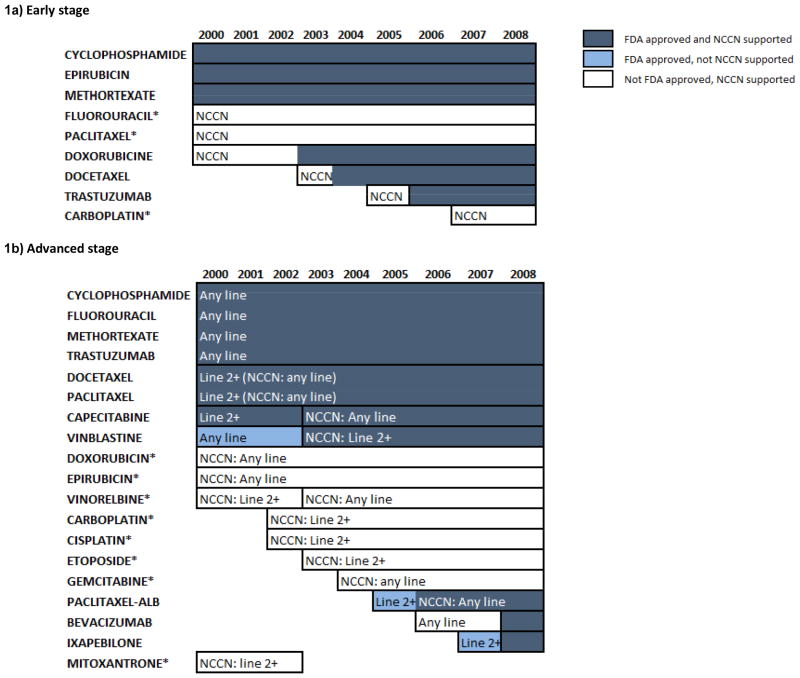
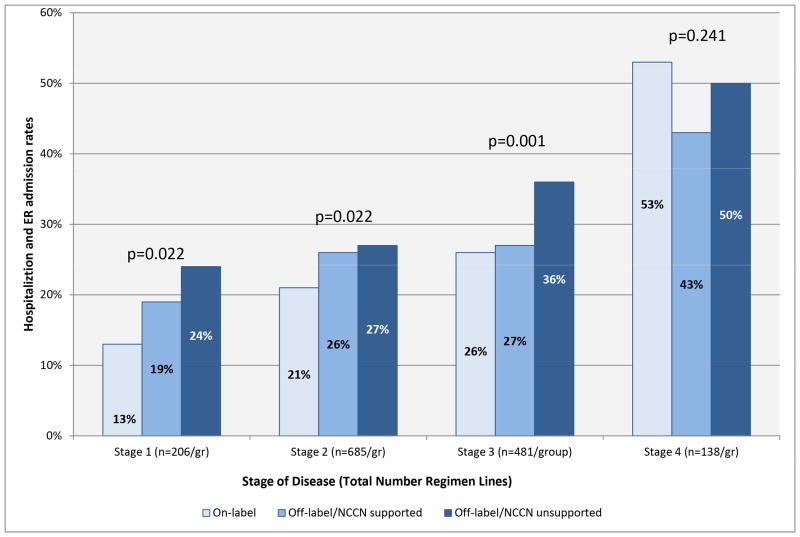
Patients and methods: The SEER-Medicare data set was used to identify women diagnosed with breast cancer. Intravenous chemotherapy was identified using Medicare claims and classified as either on-label, off-label but included in the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines) for Breast Cancer ("off-label/supported"), or off-label and not included in the NCCN Guidelines ("off-label/unsupported"). Hospitalization/emergency department (ED) admission rates were compared.
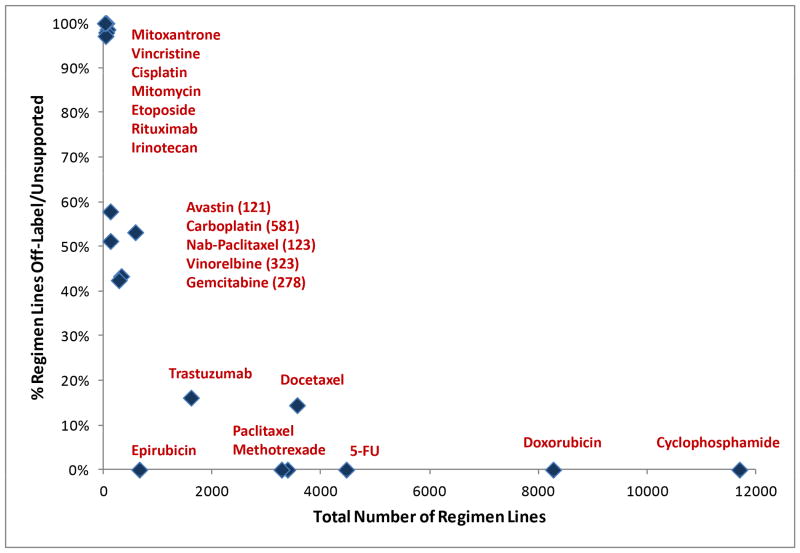
Results: A total of 13,347 women were treated with 16,127 regimens (12% of women switched regimen); 64% of regimens were off-label/supported, 25% were on-label, and 11% were off-label/unsupported, and hospitalization/ED admission occurred in 27%, 25%, and 32% of regimens, respectively (P<.0001). Drugs never included in the NCCN Guidelines for Breast Cancer accounted for 19% of off-label/unsupported use (1% of total use).
Conclusions: Off-label use without scientific support was not common, whereas 64% of use was off-label/supported, reflecting the fact that widely accepted indications are often not tested in registration trials. Off-label/supported use will likely increase as more drugs are expected to have activity across cancer sites, and therefore understanding the implications of such use is critical.
Copyright © 2016 by the National Comprehensive Cancer Network.
Figures

References
-
- Radley DC, Finkelstein SN, Stafford RS. Off-label prescribing among office-based physicians. Arch Intern Med. 2006;166:1021–6. - PubMed
-
- Stafford RS. Regulating off-label drug use- rethinking the role of the FDA. N Engl J Med. 2008;358:1427–9. - PubMed
-
- Off-label drugs. reimbursement policies constrain physicians in their choice of cancer therapies. Office USGA (ed); Washington, DC: 1991. - PubMed
-
- Scher KS, Hurria A. Under-representation of older adults in cancer registration trials: known problem, little progress. J Clin Oncol. 2012 Jun 10;30(17):2036–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
