

Large Cell Neuroendocrine Carcinoma of the Head and Neck: A Clinicopathologic Series of 10 Cases With an Emphasis on HPV Status
- PMID: 26735857
- PMCID: PMC4792746
- DOI: 10.1097/PAS.0000000000000580
Large Cell Neuroendocrine Carcinoma of the Head and Neck: A Clinicopathologic Series of 10 Cases With an Emphasis on HPV Status
Abstract
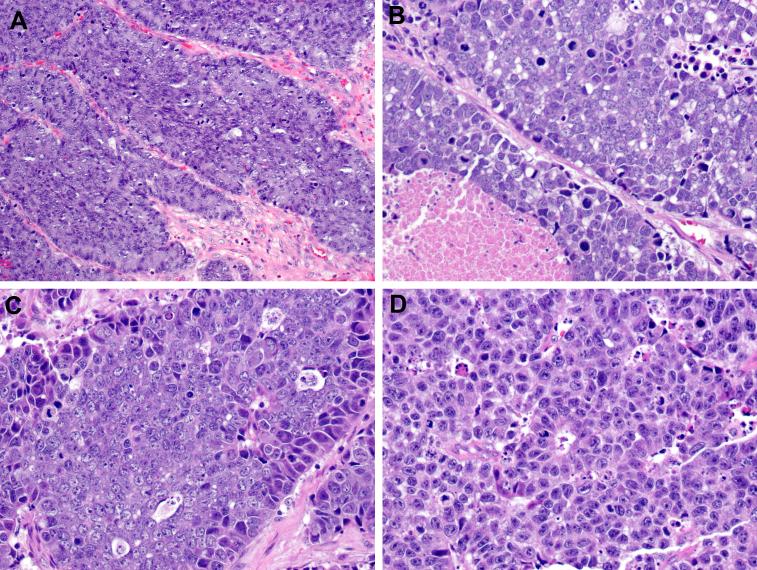
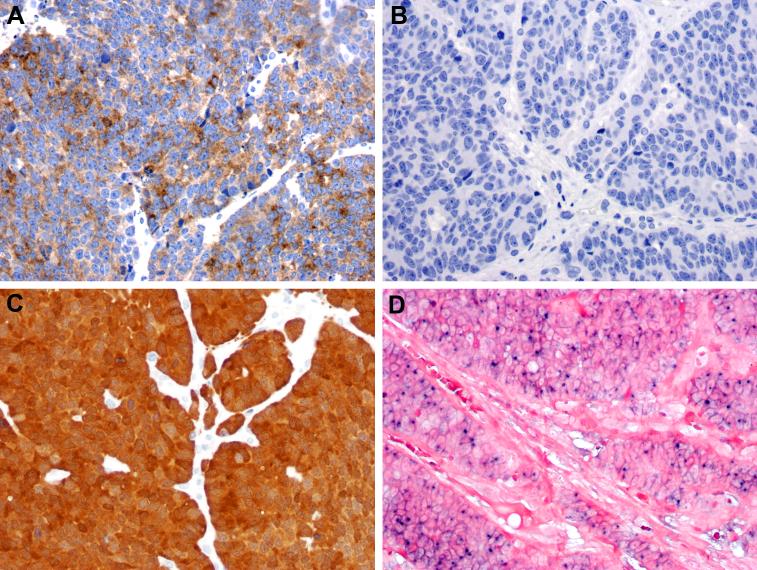
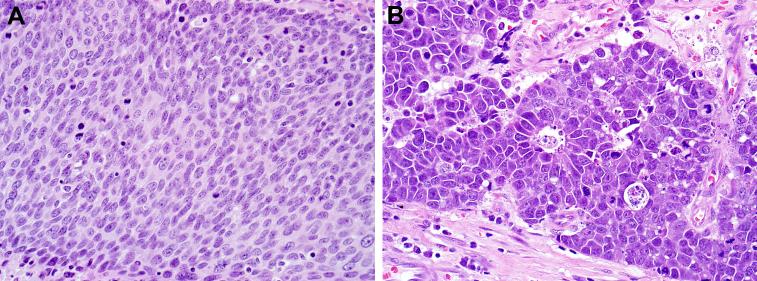
Large cell neuroendocrine carcinoma (LCNEC) is a high-grade neuroendocrine neoplasm first described in the lung and subsequently well documented in many other anatomic sites. It has only recently been recognized that LCNEC can also occasionally arise in the head and neck. The role of human papillomavirus (HPV), which is associated with some small cell carcinomas of the head and neck, has not been investigated for LCNEC. We sought to further characterize the histologic, immunophenotypic, and clinical features of LCNEC and also investigate the role of HPV in this newly described group of tumors. The surgical pathology archives of 2 large academic institutions were searched for cases of LCNEC arising in the head and neck. p16 immunohistochemistry and HPV in situ hybridization were performed, and clinical information was obtained from electronic medical records. Ten cases of head and neck LCNEC were identified. The tumors arose in 6 men and 4 women ranging in age from 14 to 70 years (median, 63.5 y). The primary tumor sites were the oropharynx (n=4), the sinonasal tract (n=3), and the larynx (n=3). The LCNECs consisted of nests and trabeculae of medium-large cells with abundant cytoplasm, coarse chromatin, and prominent nucleoli with very high mitotic rates. The tumor nests were often associated with necrosis, peripheral palisading, and rosette formations. The LCNECs were positive for pan-cytokeratin and at least 1 neuroendocrine marker (most often synaptophysin) and were largely negative for p63 (focal staining in 2/10) and CK5/6 (staining in 1/10). The LCNECs demonstrated aggressive clinical behavior: 8 of 10 presented with advanced disease, 5 of 10 died, with 4 more living but with persistent tumor. Three of 10 LCNECs were HPV-related (HPV-LCNEC); they arose in the oropharynx (n=2) and sinonasal tract (n=1). The HPV-LCNECs did not differ from the HPV-negative tumors in histologic appearance or behavior: 2 patients with HPV-LCNEC have died because of their disease and 1 remains alive but with widespread metastases. LCNEC is a rare but distinct form of head and neck carcinoma that exhibits aggressive clinical behavior. A subset of oropharyngeal and sinonasal LCNEC is HPV related, but the presence of HPV may not impart a more favorable prognosis. Because of its aggressive behavior, LCNEC should be distinguished from moderately differentiated neuroendocrine carcinoma and squamous cell carcinoma. The morphology of LCNEC overlaps considerably with the nonkeratinizing appearance of HPV-related squamous cell carcinoma, and as a result a high index of suspicion is needed to identify LCNEC. Immunohistochemical studies for synaptophysin and p63 are helpful tools for making this distinction.
Figures
References
-
- Travis WD, Linnoila RI, Tsokos MG, et al. Neuroendocrine tumors of the lung with proposed criteria for large-cell neuroendocrine carcinoma. An ultrastructural, immunohistochemical, and flow cytometric study of 35 cases. Am J Surg Pathol. 1991;15:529–553. - PubMed
-
- Jiang SX, Kameya T, Shoji M, et al. Large cell neuroendocrine carcinoma of the lung: a histologic and immunohistochemical study of 22 cases. Am J Surg Pathol. 1998;22:526–537. - PubMed
-
- Brambilla E, Beasley MB, Chirieac LR, et al. Large cell neuroendocrine carcinoma. In: Travis WD, Brambilla E, Burke AP, et al., editors. WHO Classification of Tumours of the Lung, Pleura, Thymus, and Heart. IARC Pess; Lyon, France: 2015. pp. 69–72.
-
- Barnes L, Eveson JW, Relchart P, et al. World Health Organization Classification of Tumours: Pathology and Genetics of Head and Neck Tumours. IARC Press; Lyon, France: 2005.
-
- Barnes L. Neuroendocrine tumours. In: Barnes L, Eveson JW, Reichart P, et al., editors. World Health Organization Classification of Tumours: Pathology & Genetics of Head and Neck Tumours. IARC Press; Lyon, Frane: 2005. pp. 135–139.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
