

Sources of HIV infection among men having sex with men and implications for prevention
- PMID: 26738795
- PMCID: PMC4902123
- DOI: 10.1126/scitranslmed.aad1863
Sources of HIV infection among men having sex with men and implications for prevention
Abstract
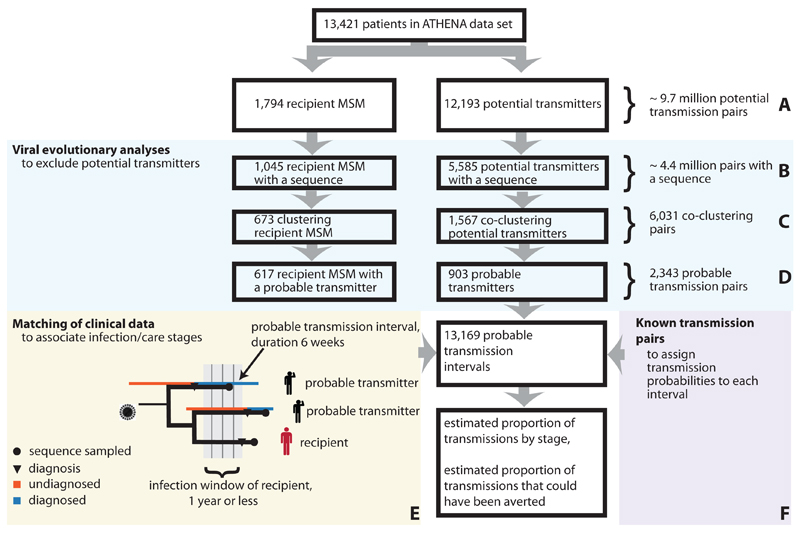
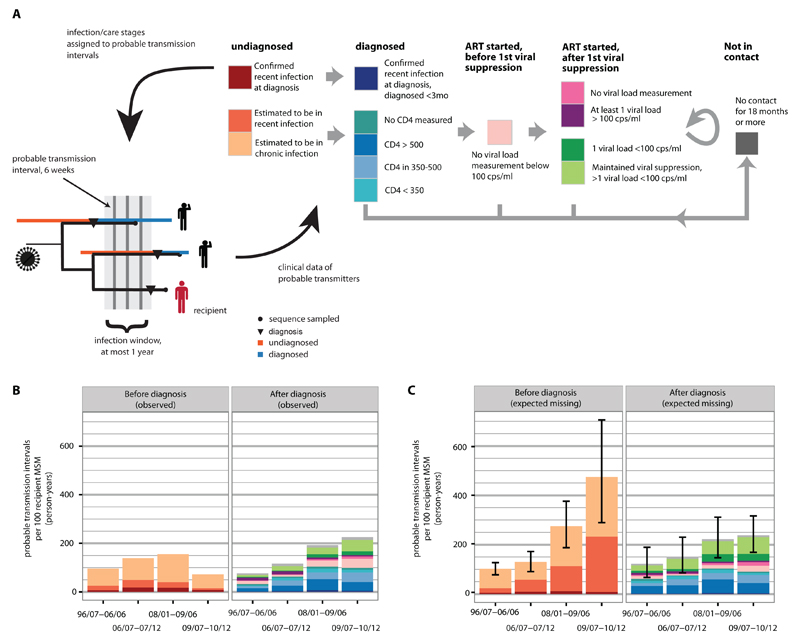
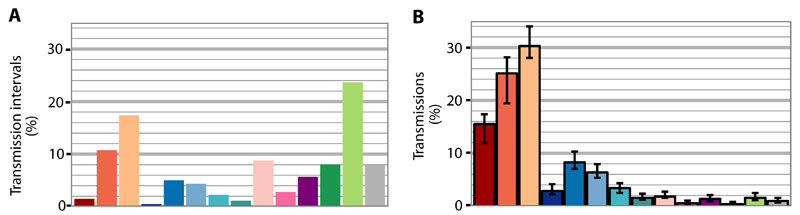
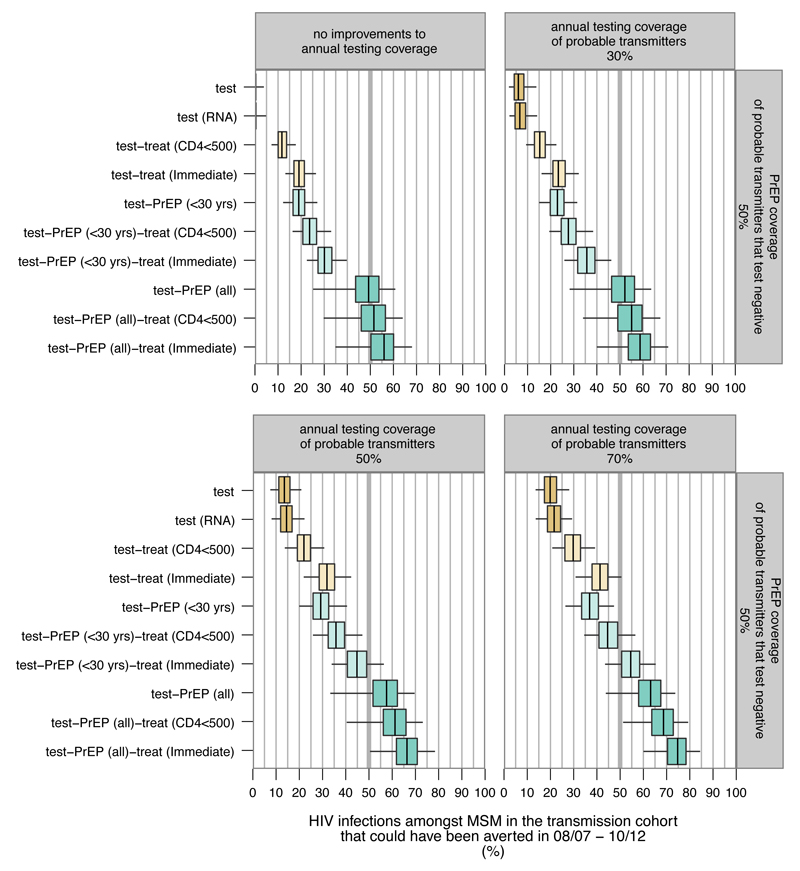
New HIV diagnoses among men having sex with men (MSM) have not decreased appreciably in most countries, even though care and prevention services have been scaled up substantially in the past 20 years. To maximize the impact of prevention strategies, it is crucial to quantify the sources of transmission at the population level. We used viral sequence and clinical patient data from one of Europe's nationwide cohort studies to estimate probable sources of transmission for 617 recently infected MSM. Seventy-one percent of transmissions were from undiagnosed men, 6% from men who had initiated antiretroviral therapy (ART), 1% from men with no contact to care for at least 18 months, and 43% from those in their first year of infection. The lack of substantial reductions in incidence among Dutch MSM is not a result of ineffective ART provision or inadequate retention in care. In counterfactual modeling scenarios, 19% of these past cases could have been averted with current annual testing coverage and immediate ART to those testing positive. Sixty-six percent of these cases could have been averted with available antiretrovirals (immediate ART provided to all MSM testing positive, and preexposure antiretroviral prophylaxis taken by half of all who test negative for HIV), but only if half of all men at risk of transmission had tested annually. With increasing sequence coverage, molecular epidemiological analyses can be a key tool to direct HIV prevention strategies to the predominant sources of infection, and help send HIV epidemics among MSM into a decisive decline.
Copyright © 2016, American Association for the Advancement of Science.
Conflict of interest statement
Figures
References
-
- Rodger A, Bruun T, Cambiano V, Vernazza P, Estrada V, Van Lunzen J, Collins S, Geretti AM, Phillips A, Lundgren J. HIV transmission risk through condomless sex if HIV+ partner on suppressive ART: PARTNER Study. 21st, Conference on Retroviruses and Opportunistic Infections; Boston, MA, USA. 2014.
-
- World Health Organization. No. September 2015. Geneva: 2015. Guideline on when to start antiretroviral therapy and on pre-exposure prophylaxis for HIV. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
