

Coronary artery bypass surgery compared with percutaneous coronary interventions in patients with insulin-treated type 2 diabetes mellitus: a systematic review and meta-analysis of 6 randomized controlled trials
- PMID: 26739589
- PMCID: PMC4702412
- DOI: 10.1186/s12933-015-0323-z
Coronary artery bypass surgery compared with percutaneous coronary interventions in patients with insulin-treated type 2 diabetes mellitus: a systematic review and meta-analysis of 6 randomized controlled trials
Abstract
Background: Data regarding the long-term clinical outcomes in patients with insulin-treated type 2 diabetes mellitus (ITDM) revascularized by either coronary artery bypass surgery (CABG) or percutaneous coronary intervention (PCI) are still controversial. We sought to compare the long-term (≥1 year) adverse clinical outcomes in patients with ITDM who underwent revascularization by either CABG or PCI.
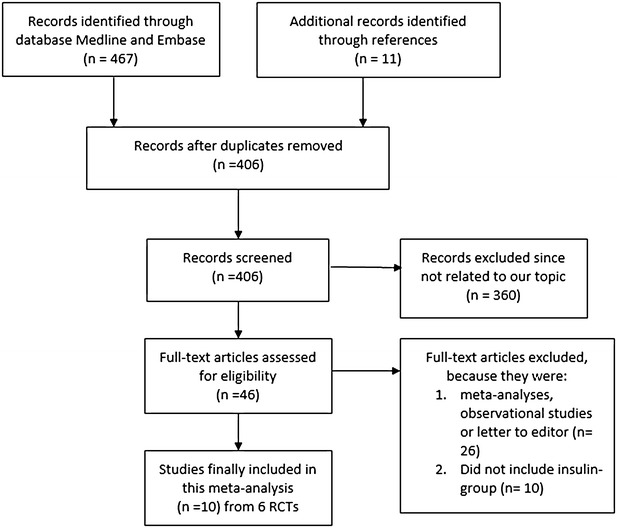
Methods: Randomized Controlled Trials (RCTs) comparing the long-term clinical outcomes in patients with ITDM and non-ITDM revascularized by either CABG or PCI were searched from electronic databases. Data for patients with ITDM were carefully retrieved. Odd Ratio (OR) with 95 % confidence interval (CI) was used to express the pooled effect on discontinuous variables and the pooled analyses were performed with RevMan 5.3.
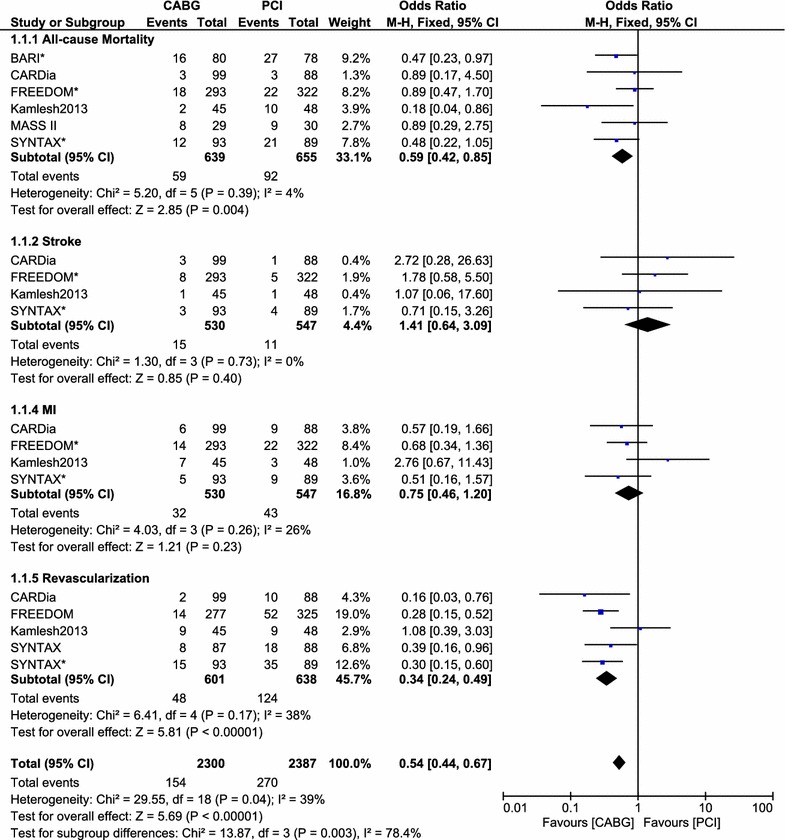
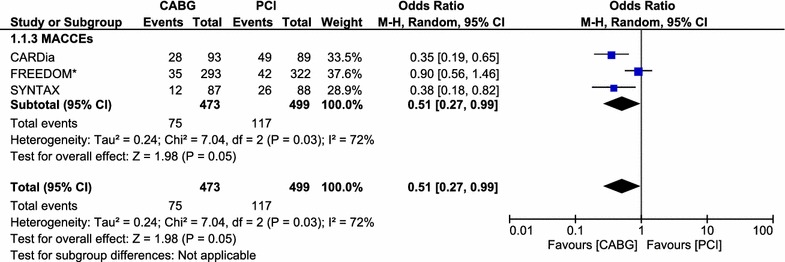
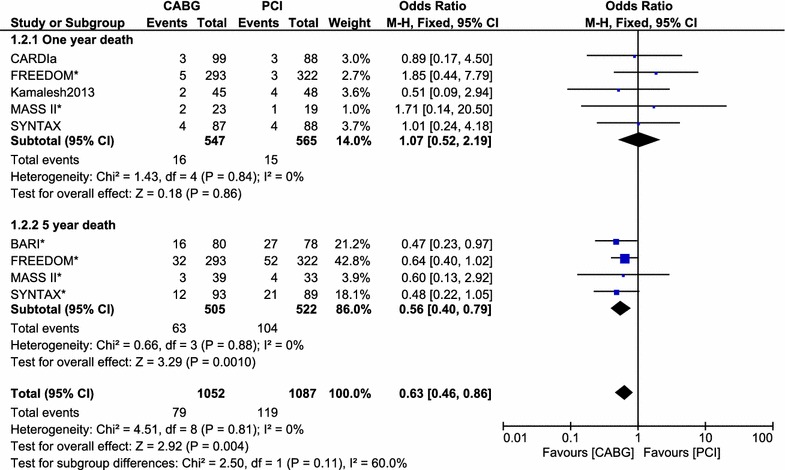
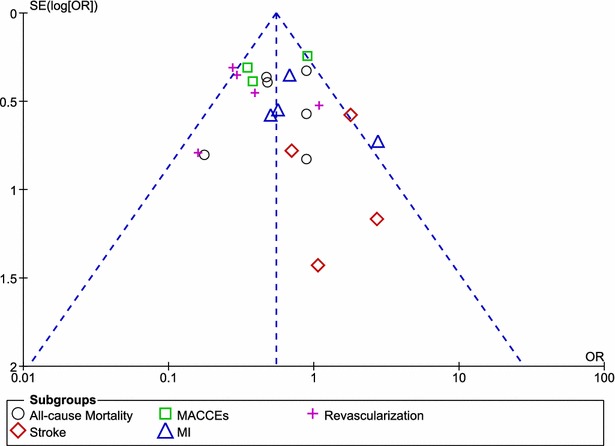
Results: Six RCTs involving 10 studies, with a total of 1297 patients with ITDM were analyzed (639 patients from the CABG group and 658 patients from the PCI group). CABG was associated with a significantly lower mortality rate compared to PCI with OR: 0.59, 95 % CI 0.42-0.85; P = 0.004. Major adverse cardiovascular and cerebrovascular events as well as repeated revascularization were also significantly lower in the CABG group with OR: 0.51, 95 % CI 0.27-0.99; P = 0.03 and OR 0.34, 95 % CI 0.24-0.49; P < 0.00001 respectively. However, compared to PCI, the rate of stroke was higher in the CABG group with OR: 1.41, 95 % CI 0.64-3.09; P = 0.40, but this result was not statistically significant.
Conclusion: CABG was associated with significantly lower long-term adverse clinical outcomes compared to PCI in patients with ITDM. However, due to an insignificantly higher rate of stroke in the CABG group, further researches with a larger number of randomized patients are required to completely solve this issue.
Figures
References
-
- Dangas GD, Farkouh ME, Sleeper LA, Yang M, Schoos MM, Macaya C, Abizaid A, Buller CE, Devlin G, Rodriguez AE, Lansky AJ, Siami FS, Domanski M, Fuster V; FREEDOM Investigators Long-term outcome of PCI versus CABG in insulin and non-insulin-treated diabetic patients: results from the FREEDOM trial. J Am Coll Cardiol. 2014;64(12):1189–1197. doi: 10.1016/j.jacc.2014.06.1182. - DOI - PubMed
-
- Kapur A, Hall RJ, Malik IS, et al. Randomized comparison of percutaneous coronary intervention with coronary artery bypass grafting in diabetic patients. 1-year results of the CARDia (Coronary Artery Revascularization in Diabetes) trial. J Am Coll Cardiol. 2010;55:432–440. doi: 10.1016/j.jacc.2009.10.014. - DOI - PubMed
-
- Sianos G, Morel MA, Kappetein AP, et al. The SYNTAX score: an angiographic tool grading the complexity of coronary artery disease. EuroIntervention. 2005;1:219–227. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
