

Efficacy and safety of nesiritide in patients with decompensated heart failure: a meta-analysis of randomised trials
- PMID: 26739721
- PMCID: PMC4716178
- DOI: 10.1136/bmjopen-2015-008545
Efficacy and safety of nesiritide in patients with decompensated heart failure: a meta-analysis of randomised trials
Abstract
Objectives: Current evidence suggests that nesiritide may have effects on renal function and decrease the incidence of mortality. However, a clear superiority using nesiritide in terms of renal toxicity and mortality in patients with heart failure was not consistently proven by previous studies. We performed a meta-analysis of all randomised trials to obtain the best estimates of efficacy and safety of nesiritide for the initial treatment of decompensated heart failure.
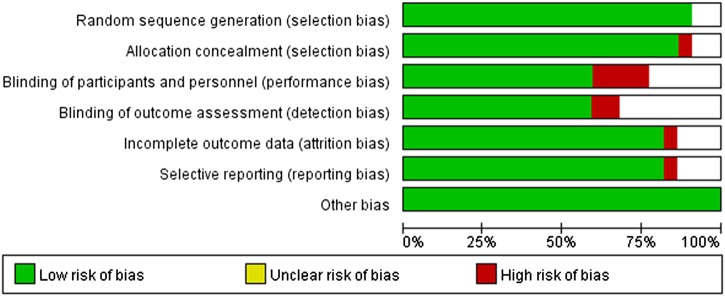
Method: We performed a meta-analysis of randomised trials of nesiritide in patients with decompensated heart failure (n=38,064 patients, in 22 trials). Two reviewers independently extracted data. Data on efficacy and safety outcomes were collected. We calculated pooled relatives risk (RRs), weighted mean difference and associated 95% CIs.
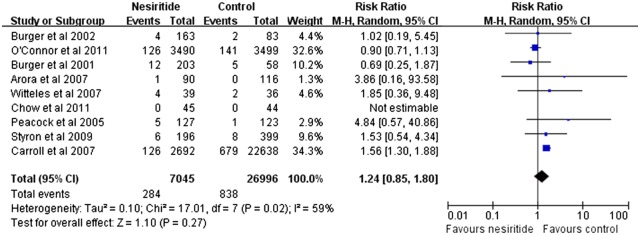
Results: Compared with placebo, dobutamine and nitroglycerin, nesiritide indicated no increasing risk of total mortality. Compared with the combined control therapy, nesiritide was associated with non-significant differences in short-term mortality (RR 1.24; 95% CI 0.85 to 1.80; p=0.27), mid-term mortality (RR 0.86; 95% CI 0.60 to 1.24; p=0.42) and long-term mortality (RR 0.94; 95% CI 0.75 to 1.18; p=0.61). Nesiritide therapy increased the risk of hypotension (p<0.00 001) and bradycardia (p=0.02) when compared with control therapy. Compared with dobutamine or placebo therapy, no differences in serum creatinine, blood urea nitrogen and creatinine clearance, and no risk of the need for dialysis was observed in nesiritide therapy.
Conclusions: Our findings indicated that, in patients with heart failure, nesiritide was not associated with the risk of mortality. However, it increased the risk of cardiovascular adverse events. The change of serum creatinine and creatinine clearance had no significant difference, and no risk of the need for dialysis was observed after low-dose nesiritide treatment.
Keywords: meta-analysis; mortality; nesiritide.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/
Figures






Similar articles
-
Short-term risk of death after treatment with nesiritide for decompensated heart failure: a pooled analysis of randomized controlled trials.JAMA. 2005 Apr 20;293(15):1900-5. doi: 10.1001/jama.293.15.1900. JAMA. 2005. PMID: 15840865
-
Nesiritide: a review of its use in acute decompensated heart failure.Drugs. 2003;63(1):47-70. doi: 10.2165/00003495-200363010-00004. Drugs. 2003. PMID: 12487622 Review.
-
Short and long-term mortality with nesiritide.Am Heart J. 2006 Dec;152(6):1084-90. doi: 10.1016/j.ahj.2006.07.002. Am Heart J. 2006. PMID: 17161057
-
Nesiritide, renal function, and associated outcomes during hospitalization for acute decompensated heart failure: results from the Acute Study of Clinical Effectiveness of Nesiritide and Decompensated Heart Failure (ASCEND-HF).Circulation. 2014 Sep 16;130(12):958-65. doi: 10.1161/CIRCULATIONAHA.113.003046. Epub 2014 Jul 29. Circulation. 2014. PMID: 25074507 Clinical Trial.
-
Nesiritide for the treatment of congestive heart failure.Expert Opin Pharmacother. 2004 Apr;5(4):901-7. doi: 10.1517/14656566.5.4.901. Expert Opin Pharmacother. 2004. PMID: 15102572 Review.
Cited by
-
Pharmacological approaches to cardio-renal syndrome: a role for the inodilator levosimendan.Eur Heart J Suppl. 2017 Mar;19(Suppl C):C22-C28. doi: 10.1093/eurheartj/sux002. Epub 2017 Mar 8. Eur Heart J Suppl. 2017. PMID: 29249907 Free PMC article.
-
Angiotensin Receptor-Neprilysin Inhibitor (ARNI) and Cardiac Arrhythmias.Int J Mol Sci. 2021 Aug 20;22(16):8994. doi: 10.3390/ijms22168994. Int J Mol Sci. 2021. PMID: 34445698 Free PMC article. Review.
-
Impact of recombinant human brain natriuretic peptide on emergency dialysis and prognosis in end-stage renal disease patients with type 4 cardiorenal syndrome.Sci Rep. 2023 Nov 25;13(1):20752. doi: 10.1038/s41598-023-48125-1. Sci Rep. 2023. PMID: 38007545 Free PMC article.
-
Nesiritide in patients with acute myocardial infarction and heart failure: a meta-analysis.J Int Med Res. 2020 Jan;48(1):300060519897194. doi: 10.1177/0300060519897194. J Int Med Res. 2020. PMID: 31948318 Free PMC article.
-
Myokine Musclin Is Critical for Exercise-Induced Cardiac Conditioning.Int J Mol Sci. 2023 Mar 30;24(7):6525. doi: 10.3390/ijms24076525. Int J Mol Sci. 2023. PMID: 37047496 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical