

A multi-factorial analysis of response to warfarin in a UK prospective cohort
- PMID: 26739746
- PMCID: PMC4702374
- DOI: 10.1186/s13073-015-0255-y
A multi-factorial analysis of response to warfarin in a UK prospective cohort
Abstract
Background: Warfarin is the most widely used oral anticoagulant worldwide, but it has a narrow therapeutic index which necessitates constant monitoring of anticoagulation response. Previous genome-wide studies have focused on identifying factors explaining variance in stable dose, but have not explored the initial patient response to warfarin, and a wider range of clinical and biochemical factors affecting both initial and stable dosing with warfarin.
Methods: A prospective cohort of 711 patients starting warfarin was followed up for 6 months with analyses focusing on both non-genetic and genetic factors. The outcome measures used were mean weekly warfarin dose (MWD), stable mean weekly dose (SMWD) and international normalised ratio (INR) > 4 during the first week. Samples were genotyped on the Illumina Human610-Quad chip. Statistical analyses were performed using Plink and R.
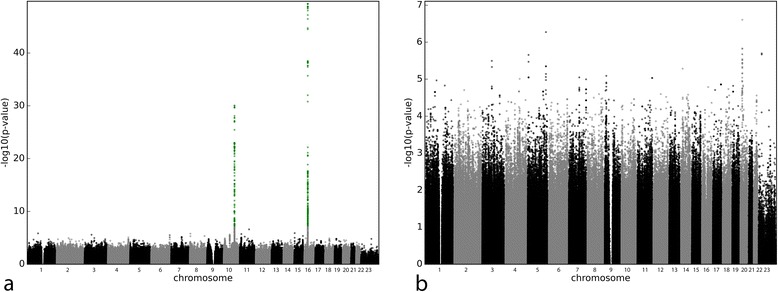
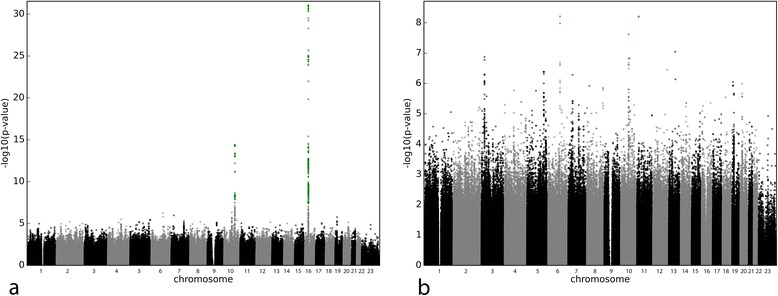
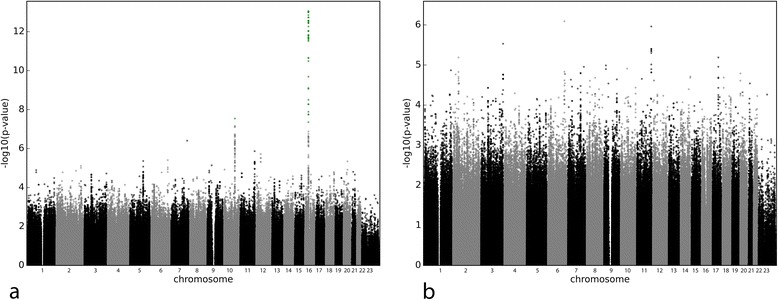
Results: VKORC1 and CYP2C9 were the major genetic determinants of warfarin MWD and SMWD, with CYP4F2 having a smaller effect. Age, height, weight, cigarette smoking and interacting medications accounted for less than 20 % of the variance. Our multifactorial analysis explained 57.89 % and 56.97 % of the variation for MWD and SMWD, respectively. Genotypes for VKORC1 and CYP2C9*3, age, height and weight, as well as other clinical factors such as alcohol consumption, loading dose and concomitant drugs were important for the initial INR response to warfarin. In a small subset of patients for whom data were available, levels of the coagulation factors VII and IX (highly correlated) also played a role.
Conclusion: Our multifactorial analysis in a prospectively recruited cohort has shown that multiple factors, genetic and clinical, are important in determining the response to warfarin. VKORC1 and CYP2C9 genetic polymorphisms are the most important determinants of warfarin dosing, and it is highly unlikely that other common variants of clinical importance influencing warfarin dosage will be found. Both VKORC1 and CYP2C9*3 are important determinants of the initial INR response to warfarin. Other novel variants, which did not reach genome-wide significance, were identified for the different outcome measures, but need replication.
Figures
References
-
- Connock M, Stevens C, Fry-Smith A, Jowett S, Fitzmaurice D, Moore D, et al. Clinical effectiveness and cost-effectiveness of different models of managing long-term oral anticoagulation therapy: a systematic review and economic modelling. Health Technol Assess. 2007;11(38):iii–iv. doi: 10.3310/hta11380. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
