

Tunnel Vision Prismatic Field Expansion: Challenges and Requirements
- PMID: 26740910
- PMCID: PMC4699714
- DOI: 10.1167/tvst.4.6.8
Tunnel Vision Prismatic Field Expansion: Challenges and Requirements
Abstract
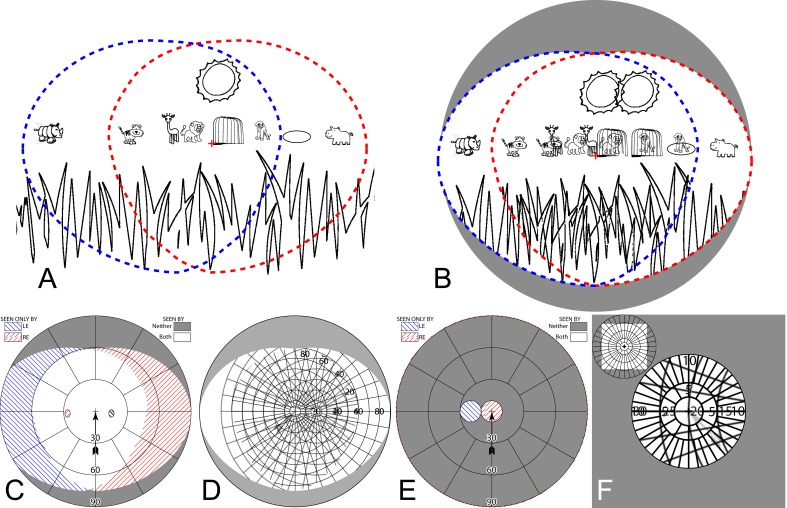
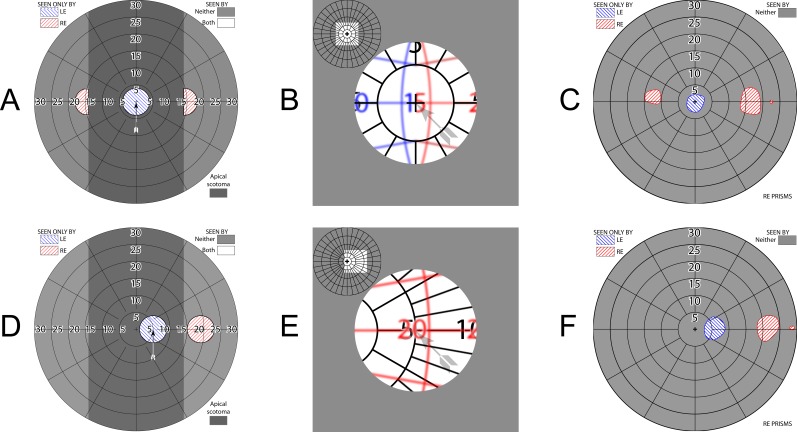
Purpose: No prismatic solution for peripheral field loss (PFL) has gained widespread acceptance. Field extended by prisms has a corresponding optical scotoma at the prism apices. True expansion can be achieved when each eye is given a different view (through visual confusion). We analyze the effects of apical scotomas and binocular visual confusion in different designs to identify constraints on any solution that is likely to meet acceptance.
Methods: Calculated perimetry diagrams were compared to perimetry with PFL patients wearing InWave channel prisms and Trifield spectacles. Percept diagrams illustrate the binocular visual confusion.
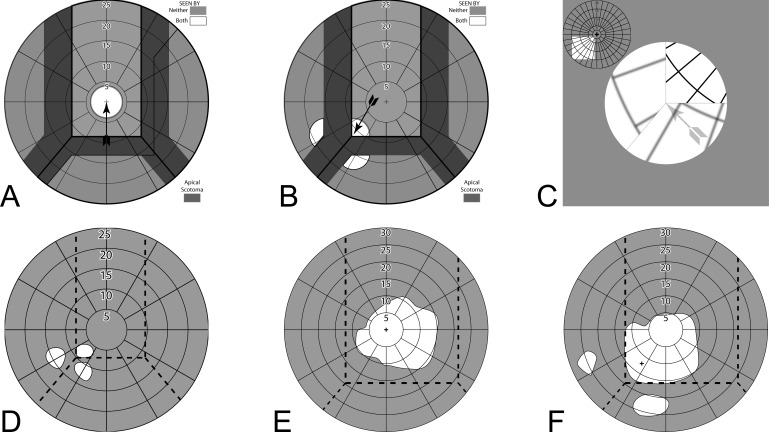
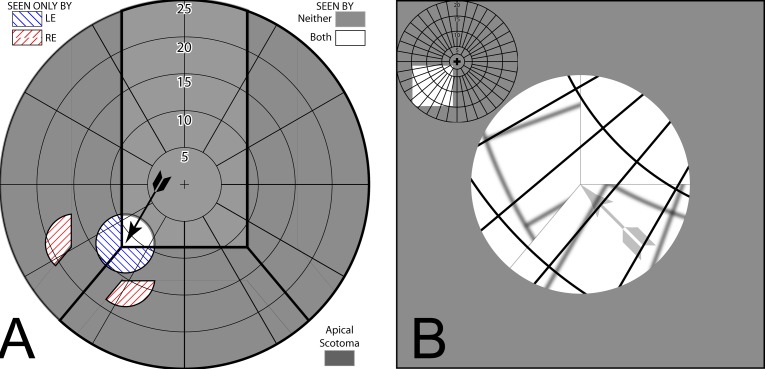
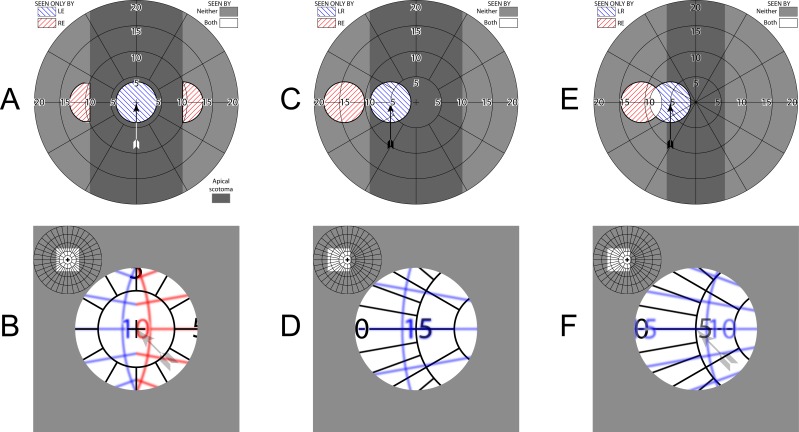
Results: Channel prisms provide no benefit at primary gaze. Inconsequential extension was provided by InWave prisms, although accessible with moderate gaze shifts. Higher-power prisms provide greater extension, with greater paracentral scotoma loss, but require uncomfortable gaze shifts. Head turns, not eye scans, are needed to see regions lost to the apical scotomas. Trifield prisms provide field expansion at all gaze positions, but acceptance was limited by disturbing effects of central binocular visual confusion.
Conclusions: Field expansion when at primary gaze (where most time is spent) is needed while still providing unobstructed central vision. Paracentral multiplexing prisms we are developing that superimpose shifted and see-through views may accomplish that.
Translational relevance: Use of the analyses and diagramming techniques presented here will be of value when considering prismatic aids for PFL, and could have prevented many unsuccessful designs and the improbable reports we cited from the literature. New designs must likely address the challenges identified here.
Keywords: low vision rehabilitation; perimetry; prism treatment; retinitis pigmentosa; tunnel vision; visual field loss.
Figures


Similar articles
-
Multiplexing Prisms for Field Expansion.Optom Vis Sci. 2017 Aug;94(8):817-829. doi: 10.1097/OPX.0000000000001102. Optom Vis Sci. 2017. PMID: 28727615 Free PMC article.
-
Considering Apical Scotomas, Confusion, and Diplopia When Prescribing Prisms for Homonymous Hemianopia.Transl Vis Sci Technol. 2013 May;2(4):2. doi: 10.1167/tvst.2.4.2. Epub 2013 May 29. Transl Vis Sci Technol. 2013. PMID: 24049719 Free PMC article.
-
High-Power Prismatic Devices for Oblique Peripheral Prisms.Optom Vis Sci. 2016 May;93(5):521-33. doi: 10.1097/OPX.0000000000000820. Optom Vis Sci. 2016. PMID: 26866438 Free PMC article.
-
Principles of modern low vision rehabilitation.Can J Ophthalmol. 2006 Jun;41(3):289-312. doi: 10.1139/I06-027. Can J Ophthalmol. 2006. PMID: 16767184 Review.
-
Central and paracentral visual field defects and driving abilities.Ophthalmologica. 2005 Jul-Aug;219(4):191-201. doi: 10.1159/000085727. Ophthalmologica. 2005. PMID: 16088237 Review.
Cited by
-
Radial and Tangential Retinal Magnifications as Functions of Visual Field Angle Across Spherical, Oblate, and Prolate Retinal Profiles.Transl Vis Sci Technol. 2022 Sep 1;11(9):10. doi: 10.1167/tvst.11.9.10. Transl Vis Sci Technol. 2022. PMID: 36121677 Free PMC article.
-
Multiplexing Prisms for Field Expansion.Optom Vis Sci. 2017 Aug;94(8):817-829. doi: 10.1097/OPX.0000000000001102. Optom Vis Sci. 2017. PMID: 28727615 Free PMC article.
-
Multi-periscopic prism device for field expansion.Biomed Opt Express. 2020 Aug 5;11(9):4872-4889. doi: 10.1364/BOE.399028. eCollection 2020 Sep 1. Biomed Opt Express. 2020. PMID: 33014587 Free PMC article.
-
Review: Binocular double vision in the presence of visual field loss.J Vis. 2024 Jun 3;24(6):13. doi: 10.1167/jov.24.6.13. J Vis. 2024. PMID: 38899959 Free PMC article. Review.
-
Peripheral Prisms Improve Obstacle Detection during Simulated Walking for Patients with Left Hemispatial Neglect and Hemianopia.Optom Vis Sci. 2018 Sep;95(9):795-804. doi: 10.1097/OPX.0000000000001280. Optom Vis Sci. 2018. PMID: 30169355 Free PMC article.
References
-
- Geruschat DR,, Turano KA. Connecting research on retinitis pigmentosa to the practice of orientation and mobility. J Vis Impair Blind. 2002; 96; 69–85.
-
- Drasdo N. Techniques instruments, cases; visual field expanders. Am J Optom Physiol Opt. 1976; 53 (9 pt 1): 464–467. - PubMed
-
- Krefman RA. Reversed telescopes on visual efficiency scores in field-restricted patients. Am J Optom Physiol Opt. 1981; 58; 159–162. - PubMed
-
- Hoeft WW,, Feinbloom W,, Brilliant R,, et al. Amorphic lenses: a mobility aid for patients with retinitis pigmentosa. Am J Optom Physiol Opt. 1985; 62: 142–148. - PubMed
-
- Szlyk JP,, Seiple W,, Laderman DJ,, Kelsch R,, Ho K,, McMahon T. Use of bioptic amorphic lenses to expand the visual field in patients with peripheral loss. Optom Vis Sci. 1998; 75; 518–524. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
