

Gossypiboma revisited: A never ending issue
- PMID: 26741272
- PMCID: PMC4756180
- DOI: 10.1016/j.ijscr.2015.12.032
Gossypiboma revisited: A never ending issue
Abstract
Introduction: Leaving a surgical item inside the patient at the end of surgery, is one of the most dreadful complications. The item is frequently a surgical sponge and the resultant morbidity is usually severe. Additionally, the event poses considerable psychic strain to the operating team, notably the surgeon.
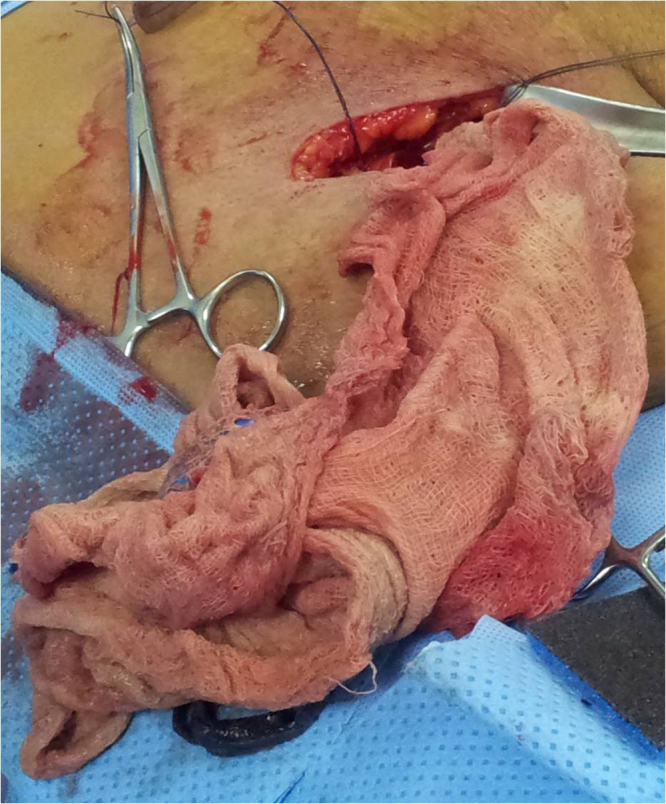
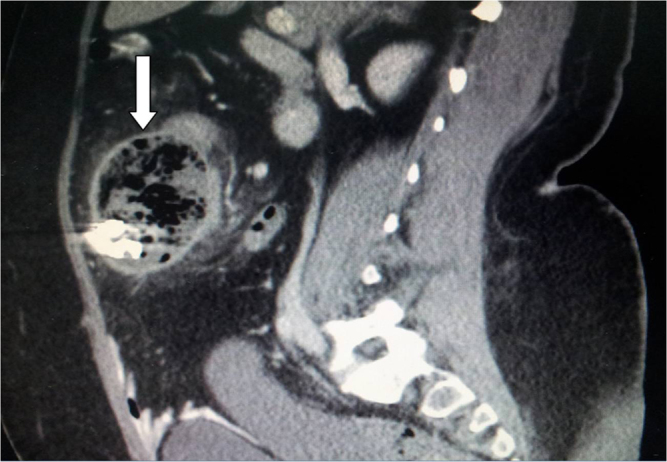
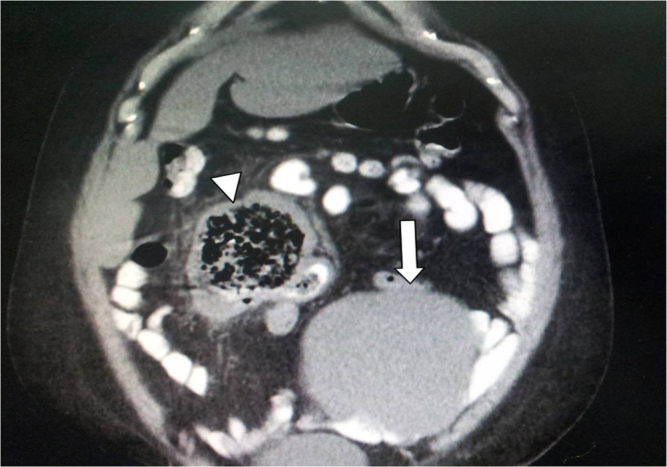
Presentation of cases: Here we describe the clinical course of three patients in whom a surgical sponge was missed, despite a seemingly correct count at the end of difficult caesarean sections. In two patients, who presented shortly after surgery, the pad was extracted with no bowel resection. In the third patient, who presented several years after surgery, colectomy was performed.
Discussion: Gossypiboma is under reported and the true incidence is largely unknown. Depending on the body reaction and the characters of the retained sponge, the patient may present within months to years after surgery. Risk factors for retained foreign objects include emergency surgery, an unplanned change in the surgical procedure, higher body mass index, multiple surgical teams, greater number of major procedures done at the same time and incorrect count recording. The surgical procedure needed to extract the retained sponge may be a simple one, as in the first case, or it may be more complex, as seen in the other two cases. Although holding the correct count at the end of surgery is the gold standard safeguard against this mishap, human errors continue to occur, as happened in our patients. For that reason, the correct count should be supplemented by employing one of the several new technologies currently available.
Conclusion: Gossypiboma continues to occur, despite precautionary measures. As its consequences might cost the patient his life and the surgeon his professional reputation, extra preventive measures should be sought and implemented. New advances in technology should be incorporated in the theatre protocol as additional safeguard against human error. When encountered, a direct incision over the encapsulated swelling, in contrast to a formal laparotomy incision, might simplify the surgical procedure.
Keywords: Gossypiboma; Prevention; Retained object.
Copyright © 2016 The Authors. Published by Elsevier Ltd.. All rights reserved.
Figures



References
-
- Cima R.R., Kollengode A., Garnatz J., Storsveen A., Weisbrod C., Deschamps C. Incidence and characteristics of potential and actual retained foreign object events in surgical patients. J. Am. Coll. Surg. 2008;207(1):80–87. - PubMed
-
- Soares F.V., Vicentini L., Dell’Aringa A.R., e Silva L.C. Textiloma in abdominal cavity: 35 years later. Arq. Bras. Cir. Dig. 2013;26(January–March (1)):74–75. - PubMed
-
- Yoon M.A., Kim E., Kwon B.J., Kim J.E., Kang H.S., Park J.H., Sohn C.H., Kim J.H., Lee D.H. Muslinoma and muslin-induced foreign body inflammatory reactions after surgical clipping and wrapping for intracranial aneurysms: imaging findings and clinical features. J. Neurosurg. 2010;112(March (3)):640–647. - PubMed
-
- Kawahara S., Honda M., Kosuda S., Tamura K., Miwa K., Hashimoto T., Nobusawa H., Satoh S., Ootsuki N., Gokan T. CT and US findings of gauzeoma. Nihon Igaku Hoshasen Gakkai Zasshi. 1990;50(April (4)):375–381. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
