

Renal artery stenosis: if and when to intervene
- PMID: 26741885
- PMCID: PMC4768864
- DOI: 10.1097/MNH.0000000000000202
Renal artery stenosis: if and when to intervene
Abstract
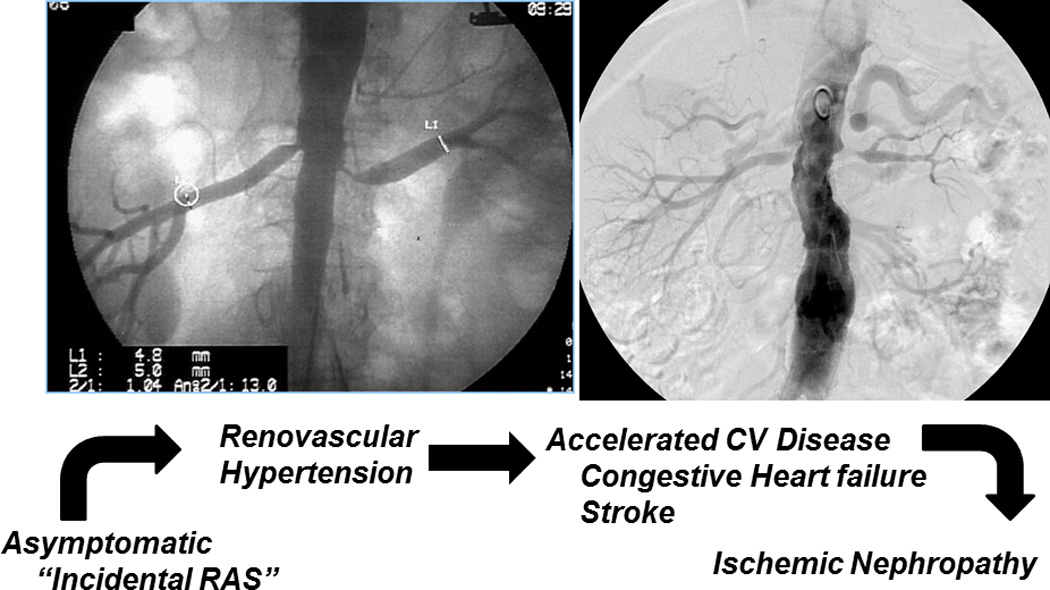
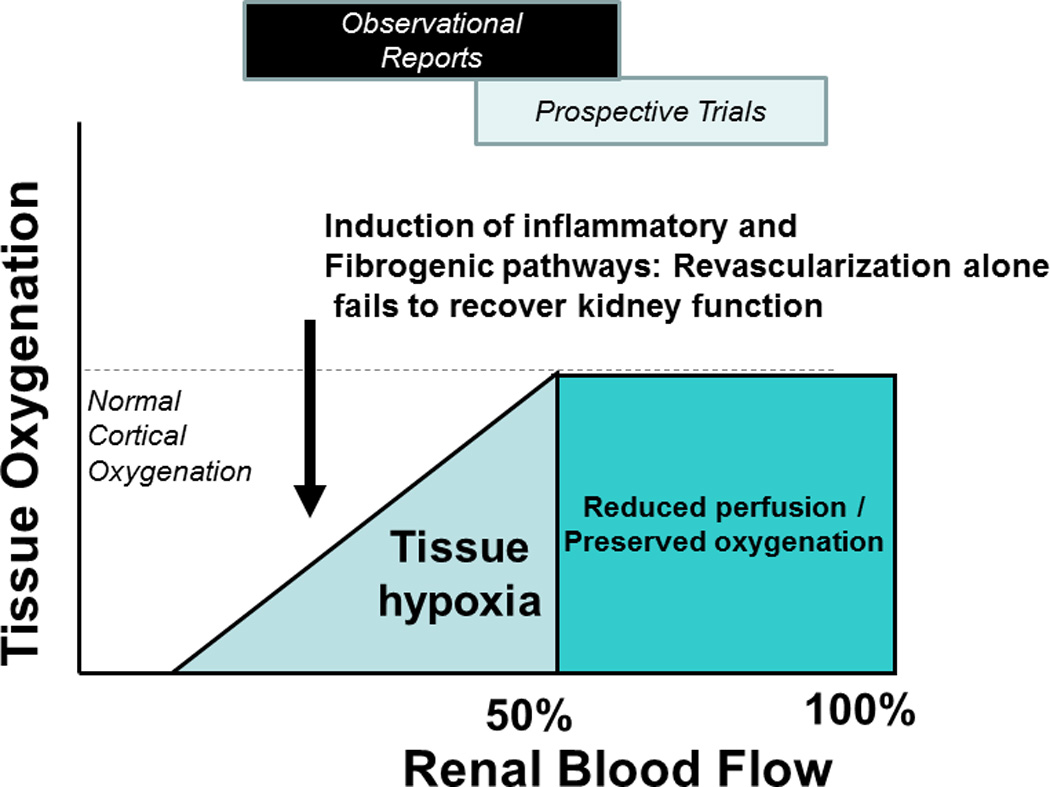
Purpose of review: Atherosclerotic renovascular disease remains highly prevalent and presents an array of clinical syndromes. Recent prospective trials have dampened enthusiasm for revascularization generally, but clinicians recognize the need to identify patients likely to benefit from vascular intervention.
Recent findings: This article highlights the inflammatory nature of vascular occlusive disease and the limits of the kidney to adapt to reduced blood flow. Although moderate reductions can be tolerated, severe impairment of renal perfusion leads to tissue hypoxia and activates inflammatory injury within the kidney. Hence, assessment of kidney viability and potential tools to modify mitochondrial and inflammatory damage may be important to identify patients for whom clinical intervention should be undertaken.
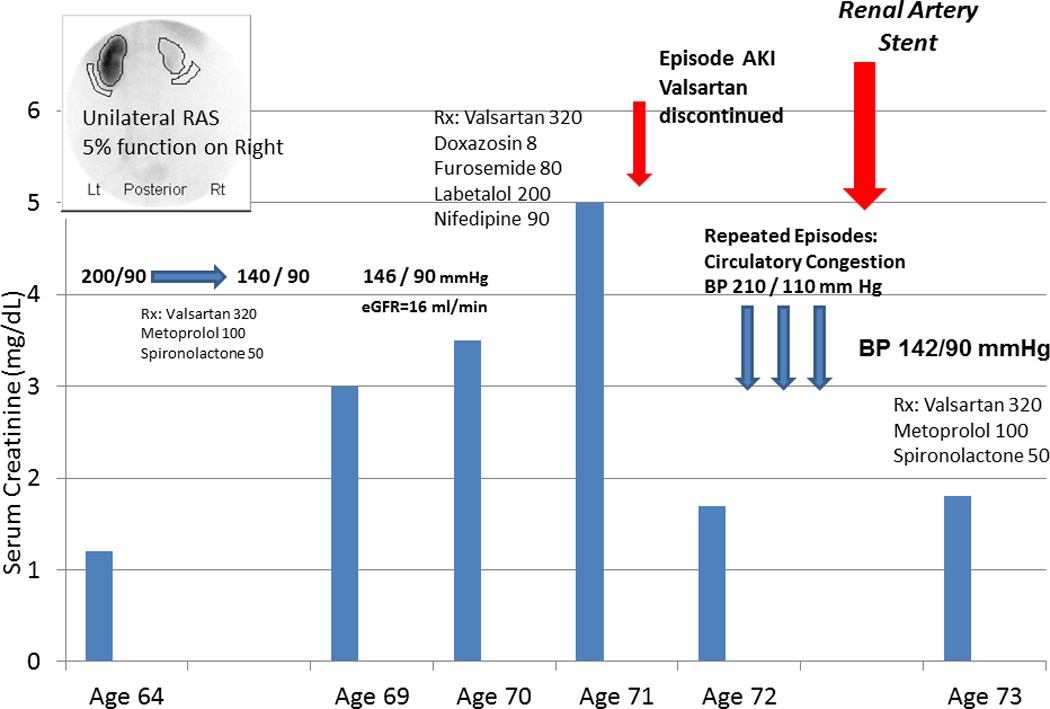
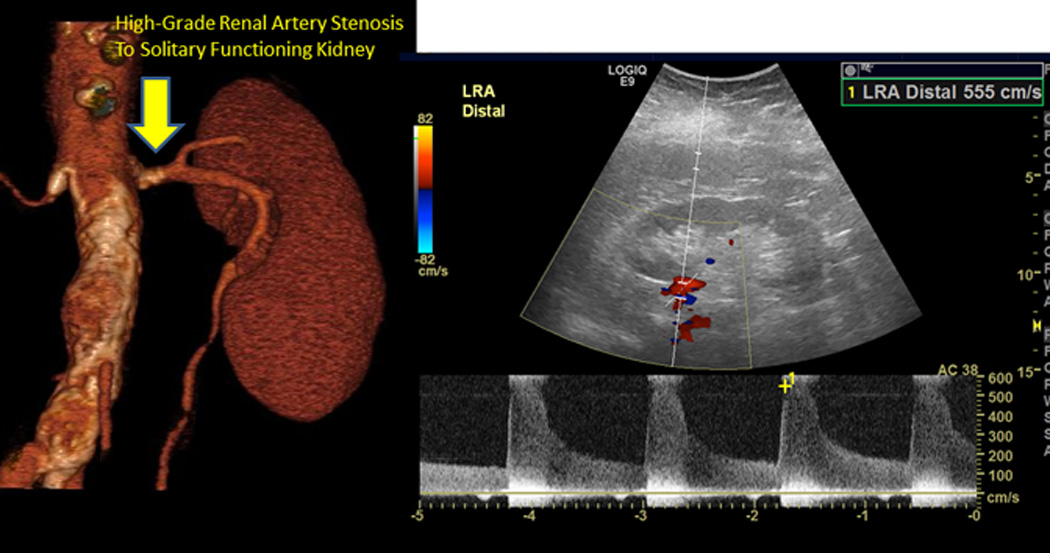
Summary: Clinicians must recognize clinical syndromes that identify 'high-risk' groups and apply revascularization in those likely to benefit. Future efforts to protect the kidney (e.g., mitochondrial protection) or cell-based therapy may amplify clinical recovery when combined with restoring renal blood flow.
Conflict of interest statement
Figures
References
-
- Mark PB, Schiffrin EL, Jennings GL, et al. Renovascular hypertension: to stent or not to stent? Hypertension. 2014;64:1165–1168. - PubMed
-
-
Herrmann SM, Saad A, Textor SC. Management of atherosclerotic renovascular disease after Cardiovascular Outcomes in Renal Atherosclerotic Lesions (CORAL) Nephrology, dialysis, transplantation : official publication of the European Dialysis and Transplant Association - European Renal Association. 2015;30:366–375. Review of trials with exploration of limited entry criteria and selection bias that limits generalizability in clinical practice.
-
-
-
Ritchie J, Green D, Chrysochou C, et al. High-risk clinical presentations in atherosclerotic renovascular disease: prognosis and response to renal artery revascularization. American journal of kidney diseases : the official journal of the National Kidney Foundation. 2014;63:186–197. Important identification of “high-risk” subsets from an regional database for atherosclerotic renovascular disease in the United Kingdom. These authors identified clinical syndromes of episodic pulmonary edema and rapidly progressive renal failure with severe hypertension for which renal revascularization confered important survival benefits.
-
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
