

Arsenic Trioxide as a Radiation Sensitizer for 131I-Metaiodobenzylguanidine Therapy: Results of a Phase II Study
- PMID: 26742708
- PMCID: PMC4976822
- DOI: 10.2967/jnumed.115.161752
Arsenic Trioxide as a Radiation Sensitizer for 131I-Metaiodobenzylguanidine Therapy: Results of a Phase II Study
Abstract
Arsenic trioxide has in vitro and in vivo radiosensitizing properties. We hypothesized that arsenic trioxide would enhance the efficacy of the targeted radiotherapeutic agent (131)I-metaiodobenzylguanidine ((131)I-MIBG) and tested the combination in a phase II clinical trial.
Methods: Patients with recurrent or refractory stage 4 neuroblastoma or metastatic paraganglioma/pheochromocytoma (MP) were treated using an institutional review board-approved protocol (Clinicaltrials.gov identifier NCT00107289). The planned treatment was (131)I-MIBG (444 or 666 MBq/kg) intravenously on day 1 plus arsenic trioxide (0.15 or 0.25 mg/m(2)) intravenously on days 6-10 and 13-17. Toxicity was evaluated using National Cancer Institute Common Toxicity Criteria, version 3.0. Response was assessed by International Neuroblastoma Response Criteria or (for MP) by changes in (123)I-MIBG or PET scans.
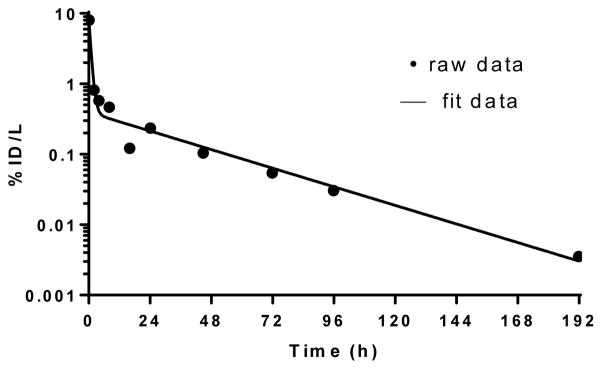
Results: Twenty-one patients were treated: 19 with neuroblastoma and 2 with MP. Fourteen patients received (131)I-MIBG and arsenic trioxide, both at maximal dosages; 2 patients received a 444 MBq/kg dose of (131)I-MIBG plus a 0.15 mg/kg dose of arsenic trioxide; and 3 patients received a 666 MBq/kg dose of (131)I-MIBG plus a 0.15 mg/kg dose of arsenic trioxide. One did not receive arsenic trioxide because of transient central line-induced cardiac arrhythmia, and another received only 6 of 10 planned doses of arsenic trioxide because of grade 3 diarrhea and vomiting with concurrent grade 3 hypokalemia and hyponatremia. Nineteen patients experienced myelosuppression higher than grade 2, most frequently thrombocytopenia (n = 18), though none required autologous stem cell rescue. Twelve of 13 evaluable patients experienced hyperamylasemia higher than grade 2 from transient sialoadenitis. By International Neuroblastoma Response Criteria, 12 neuroblastoma patients had no response and 7 had progressive disease, including 6 of 8 entering the study with progressive disease. Objective improvements in semiquantitative (131)I-MIBG scores were observed in 6 patients. No response was seen in MP. Seventeen of 19 neuroblastoma patients continued on further chemotherapy or immunotherapy. Mean 5-year overall survival (±SD) for neuroblastoma was 37% ± 11%. Mean absorbed dose of (131)I-MIBG to blood was 0.134 cGy/MBq, well below myeloablative levels in all patients.
Conclusion: (131)I-MIBG plus arsenic trioxide was well tolerated, with an adverse event profile similar to that of (131)I-MIBG therapy alone. The addition of arsenic trioxide to (131)I-MIBG did not significantly improve response rates when compared with historical data with (131)I-MIBG alone.
Keywords: MIBG therapy; malignant pheochromocytoma/paraganglioma; neuroblastoma; radiosensitization.
© 2016 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
Conflict of interest statement
Figures
References
-
- Wieland DM, Wu J, Brown LE, Mangner TJ, Swanson DP, Beierwaltes WH. Radiolabeled adrenergi neuron-blocking agents: adrenomedullary imaging with [131I]iodobenzylguanidine. J Nucl Med. 1980;21:349–353. - PubMed
-
- Modak S, Cheung NK. Neuroblastoma: Therapeutic strategies for a clinical enigma. Cancer Treat Rev. 2010;36:307–317. - PubMed
-
- Kushner BH. Neuroblastoma: a disease requiring a multitude of imaging studies. J Nucl Med. 2004;45:1172–1188. - PubMed
-
- Wilson JS, Gains JE, Moroz V, Wheatley K, Gaze MN. A systematic review of 131I-meta iodobenzylguanidine molecular radiotherapy for neuroblastoma. Eur J Cancer. 2014;50:801–815. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical