

Enhanced engraftment, proliferation, and therapeutic potential in heart using optimized human iPSC-derived cardiomyocytes
- PMID: 26743035
- PMCID: PMC4705488
- DOI: 10.1038/srep19111
Enhanced engraftment, proliferation, and therapeutic potential in heart using optimized human iPSC-derived cardiomyocytes
Abstract
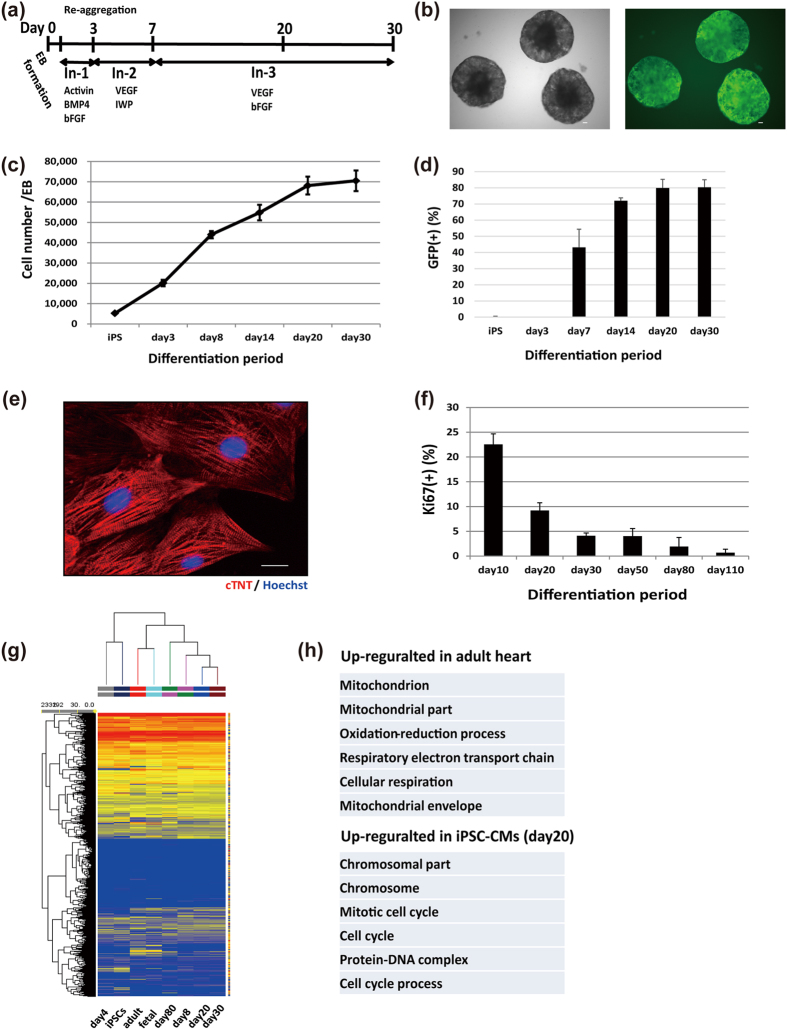
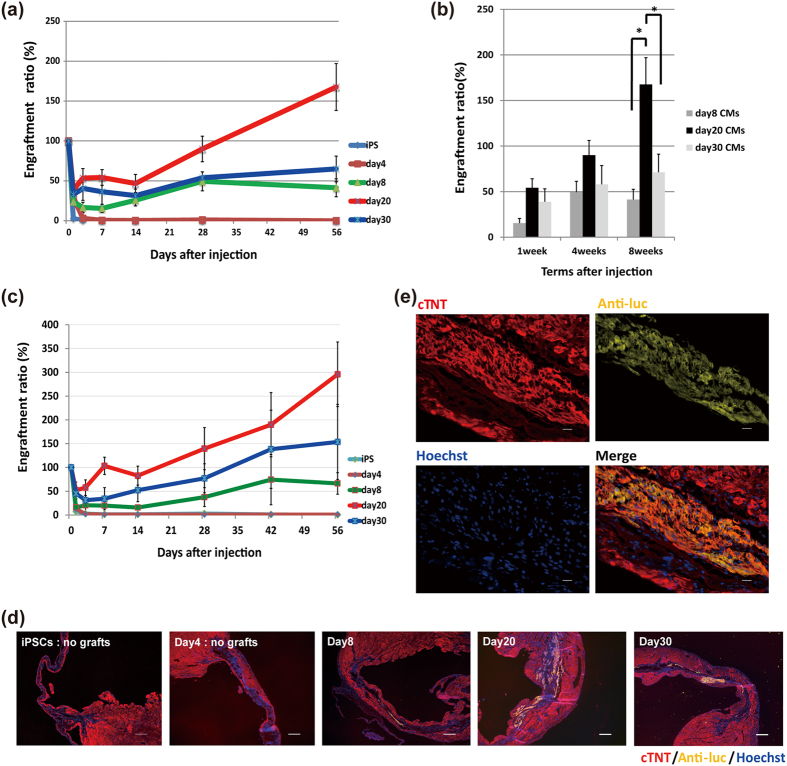
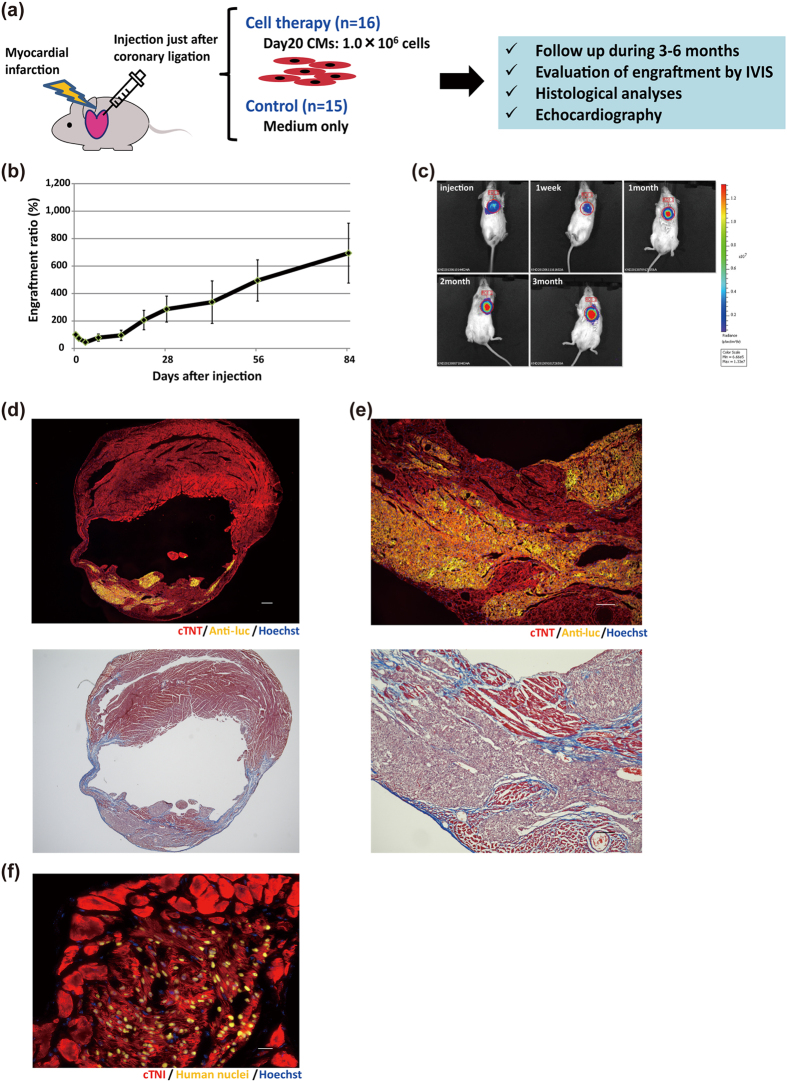
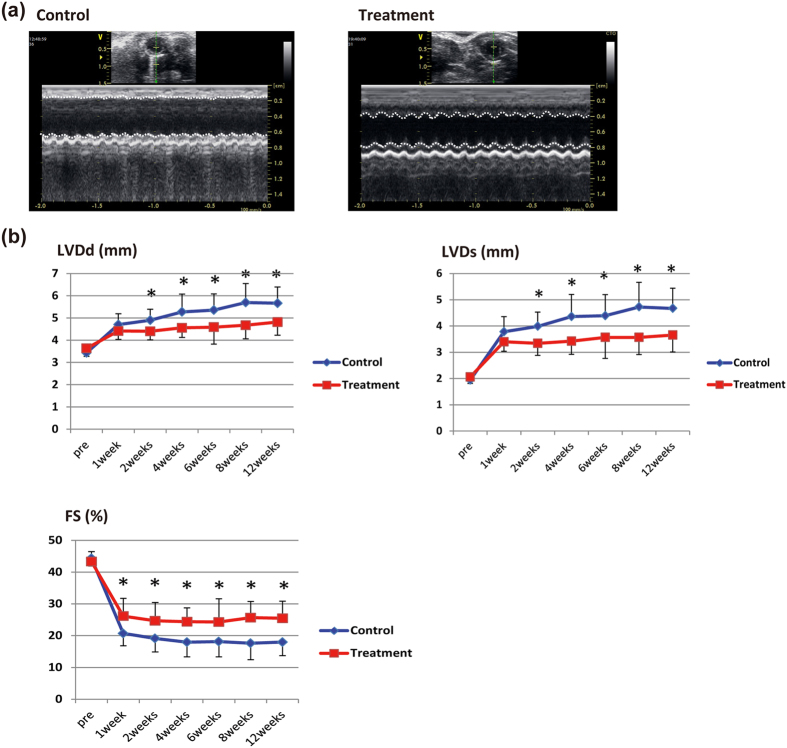
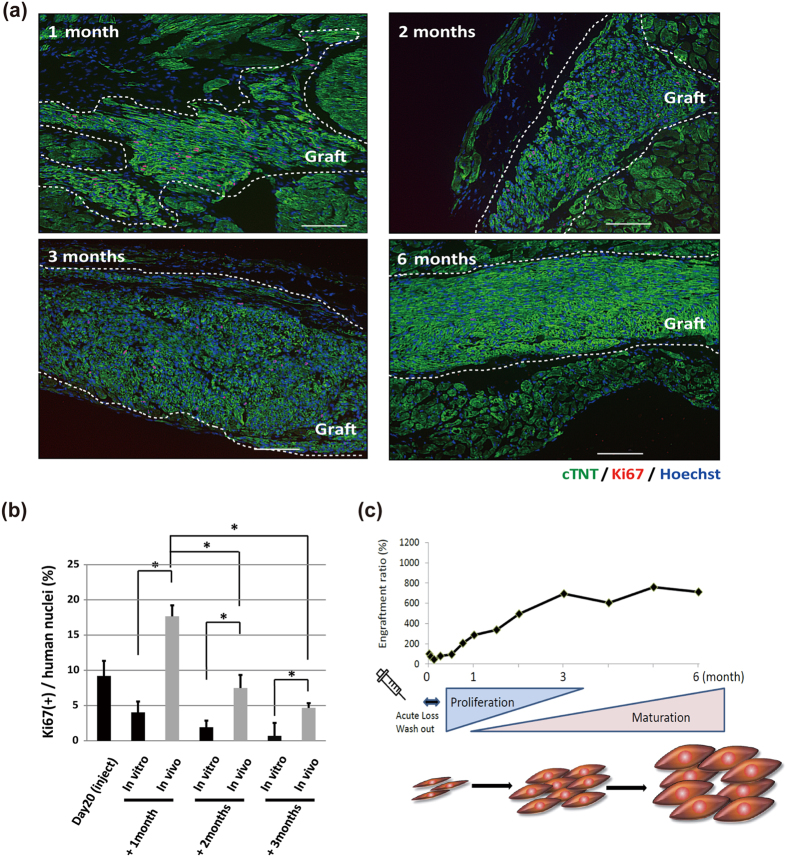
Human pluripotent stem cell-derived cardiomyocytes (CMs) are a promising tool for cardiac cell therapy. Although transplantation of induced pluripotent stem cell (iPSC)-derived CMs have been reported in several animal models, the treatment effect was limited, probably due to poor optimization of the injected cells. To optimize graft cells for cardiac reconstruction, we compared the engraftment efficiency of intramyocardially-injected undifferentiated-iPSCs, day 4 mesodermal cells, and day 8, day 20, and day 30 purified iPSC-CMs after initial differentiation by tracing the engraftment ratio (ER) using in vivo bioluminescence imaging. This analysis revealed the ER of day 20 CMs was significantly higher compared to other cells. Transplantation of day 20 CMs into the infarcted hearts of immunodeficient mice showed good engraftment, and echocardiography showed significant functional improvement by cell therapy. Moreover, the imaging signal and ratio of Ki67-positive CMs at 3 months post injection indicated engrafted CMs proliferated in the host heart. Although this graft growth reached a plateau at 3 months, histological analysis confirmed progressive maturation from 3 to 6 months. These results suggested that day 20 CMs had very high engraftment, proliferation, and therapeutic potential in host mouse hearts. They also demonstrate this model can be used to track the fate of transplanted cells over a long time.
Conflict of interest statement
S.Y. is a scientific advisor of iPS Academia Japan without salary.
Figures


References
-
- Stehlik J. et al. The Registry of the International Society for Heart and Lung Transplantation: Twenty-eighth Adult Heart Transplant Report–2011. The Journal of heart and lung transplantation: the official publication of the International Society for Heart Transplantation 30, 1078–1094 (2011). - PubMed
-
- Ptaszek L. M., Mansour M., Ruskin J. N. & Chien K. R. Towards regenerative therapy for cardiac disease. Lancet 379, 933–942 (2012). - PubMed
-
- Malliaras K. et al. Intracoronary cardiosphere-derived cells after myocardial infarction: evidence of therapeutic regeneration in the final 1-year results of the CADUCEUS trial (CArdiosphere-Derived aUtologous stem CElls to reverse ventricUlar dySfunction). Journal of the American College of Cardiology 63, 110–122 (2014). - PMC - PubMed
-
- Schachinger V. et al. Intracoronary bone marrow-derived progenitor cells in acute myocardial infarction. N Engl J Med 355, 1210–1221 (2006). - PubMed
-
- Tendera M. et al. Intracoronary infusion of bone marrow-derived selected CD34+CXCR4+ cells and non-selected mononuclear cells in patients with acute STEMI and reduced left ventricular ejection fraction: results of randomized, multicentre Myocardial Regeneration by Intracoronary Infusion of Selected Population of Stem Cells in Acute Myocardial Infarction (REGENT) Trial. Eur Heart J 30, 1313–1321 (2009). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
