

Influence of different electrode belt positions on electrical impedance tomography imaging of regional ventilation: a prospective observational study
- PMID: 26743570
- PMCID: PMC4705633
- DOI: 10.1186/s13054-015-1161-9
Influence of different electrode belt positions on electrical impedance tomography imaging of regional ventilation: a prospective observational study
Abstract
Background: Electrical impedance tomography (EIT) is a non-invasive bedside tool which allows an individualized ventilator strategy by monitoring tidal ventilation and lung aeration. EIT can be performed at different cranio-caudal thoracic levels, but data are missing about the optimal belt position. The main goal of this prospective observational study was to evaluate the impact of different electrode layers on tidal impedance variation in relation to global volume changes in order to propose a proper belt position for EIT measurements.
Methods: EIT measurements were performed in 15 mechanically ventilated intensive care patients with the electrode belt at different thoracic layers (L1-L7). All respiratory and hemodynamic parameters were recorded. Blood gas analyses were obtained once at the beginning of EIT examination. Off-line tidal impedance variation/tidal volume (TV/VT) ratio was calculated, and specific patterns of impedance distribution due to automatic and user-defined adjustment of the colour scale for EIT images were identified.
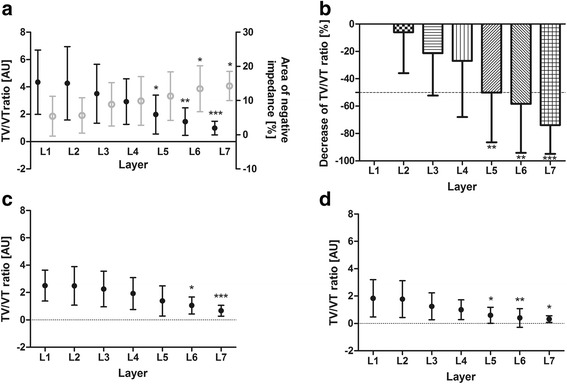
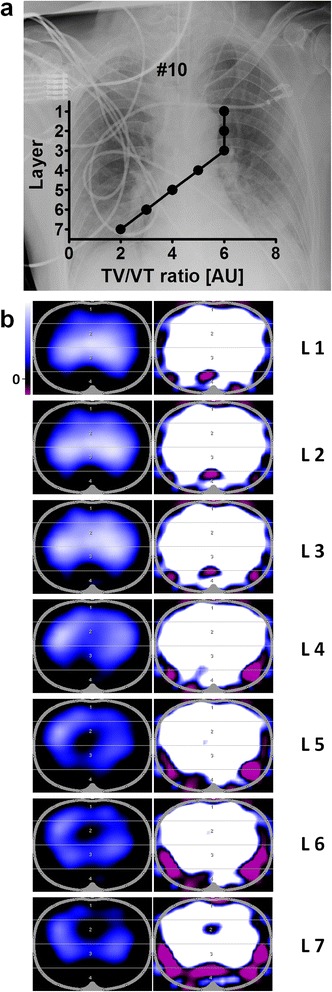
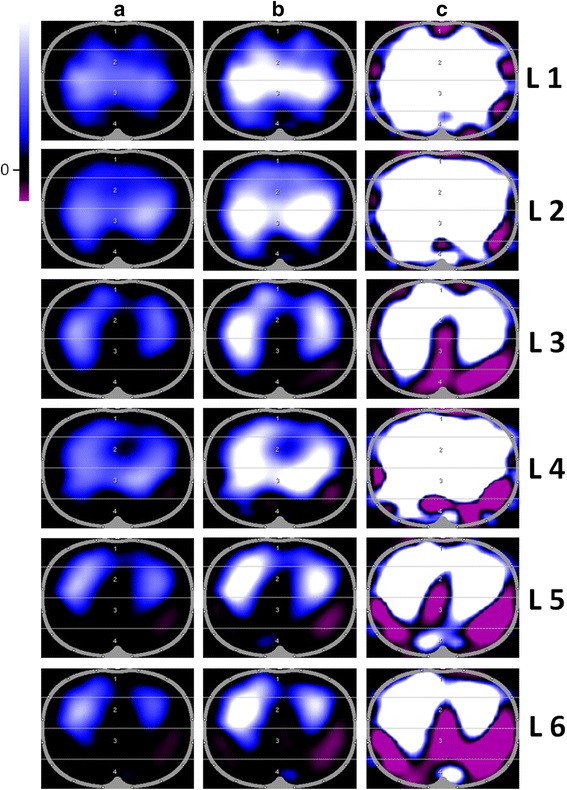
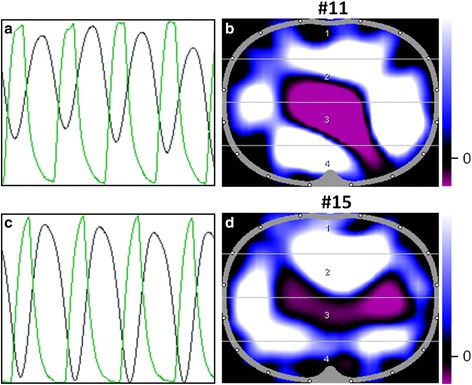
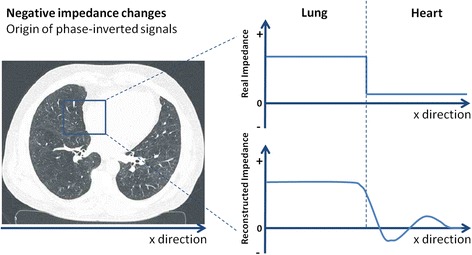
Results: TV/VT ratio is the highest at L1. It decreases in caudal direction. At L5, the decrease of TV/VT ratio is significant. We could identify patterns of diaphragmatic interference with ventilation-related impedance changes, which owing to the automatically adjusted colour scales are not obvious in the regularly displayed EIT images.
Conclusions: The clinical usability and plausibility of EIT measurements depend on proper belt position, proper impedance visualisation, correct analysis and data interpretation. When EIT is used to estimate global parameters like VT or changes in end-expiratory lung volume, the best electrode plane is between the 4th and 5th intercostal space. The specific colour coding occasionally suppresses user-relevant information, and manual rescaling of images is necessary to visualise this information.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
