

Clinical inertia with regard to intensifying therapy in people with type 2 diabetes treated with basal insulin
- PMID: 26743666
- PMCID: PMC5067688
- DOI: 10.1111/dom.12626
Clinical inertia with regard to intensifying therapy in people with type 2 diabetes treated with basal insulin
Abstract
Aim: To investigate whether clinical inertia, the failure to intensify treatment regimens when required, exists in people with type 2 diabetes treated with basal insulin.
Methods: This was a retrospective cohort study involving patients with type 2 diabetes in the UK Clinical Practice Research Datalink database between January 2004 and December 2011, with follow-up until December 2013.
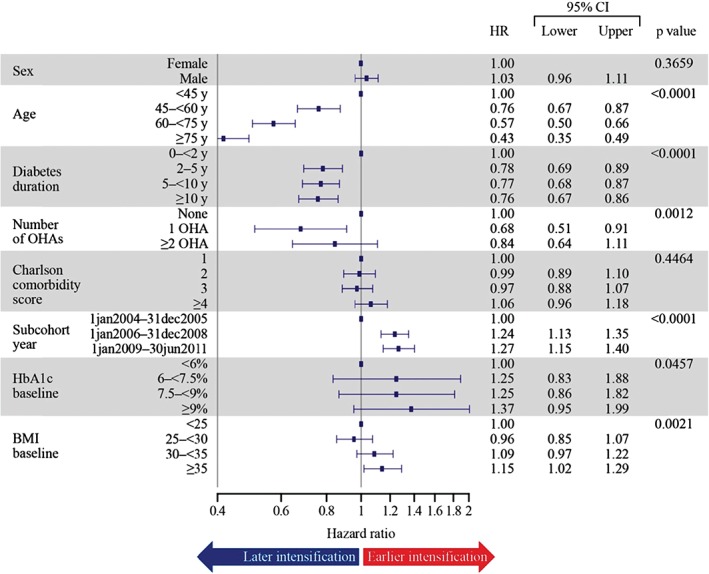
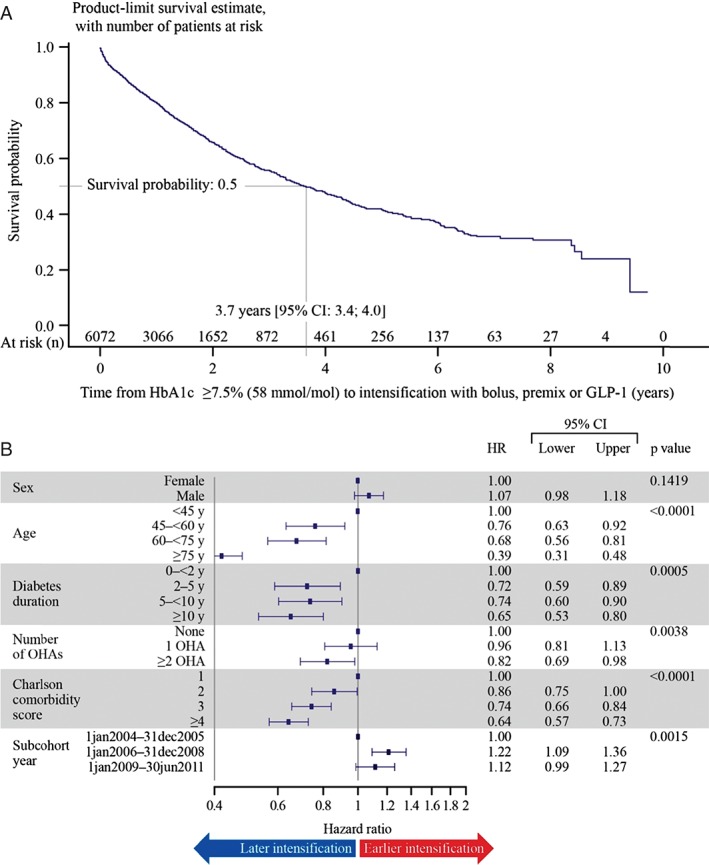
Results: A total of 11 696 patients were included in the analysis. Among all patients, 36.5% had their treatment intensified during the study period; of these, the treatment of 50.0, 42.5 and 7.4% was intensified with bolus or premix insulin or glucagon-like peptide-1 receptor agonists, respectively. The median time from initiation of basal insulin to treatment intensification was 4.3 years [95% confidence interval (CI) 4.1, 4.6]. Among patients clinically eligible for treatment intensification [glycated haemoglobin (HbA1c) ≥7.5% (58 mmol/mol)], 30.9% had their treatment regimen intensified. The median time to intensification in this group was 3.7 years (95% CI 3.4, 4.0). Increasing age, duration of diabetes, oral antihyperglycaemic agent usage and Charlson comorbidity index score were associated with a significant delay in the time to intensification (p < 0.05). Among patients with HbA1c ≥7.5% (58 mmol/mol), 32.1% stopped basal insulin therapy.
Conclusions: Strategies should be developed to increase the number of patients undergoing therapy intensification and to reduce the delay in intensifying therapy for suitable patients on basal insulin. Initiatives to support patients continuing on insulin are also required.
Keywords: basal; glucagon-like peptide-1; glycaemic control; intensive insulin therapy; type 2 diabetes.
© 2016 The Authors. Diabetes, Obesity and Metabolism published by John Wiley & Sons Ltd.
Figures
References
-
- American Diabetes Association . Standards of medical care in diabetes—2014. Diabetes Care 2014; 37(Suppl. 1): S14–80. - PubMed
-
- Inzucchi SE, Bergenstal RM, Buse JB et al. Management of hyperglycemia in type 2 diabetes, 2015: a patient‐centered approach: update to a position statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care 2015; 38: 140–149. - PubMed
-
- Chatterton H, Younger T, Fischer A, Khunti K; Programme development group. Risk identification and interventions to prevent type 2 diabetes in adults at high risk: summary of NICE guidance. BMJ 2012; 345: e4624. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
