

Computational Identification of Tumor Anatomic Location Associated with Survival in 2 Large Cohorts of Human Primary Glioblastomas
- PMID: 26744442
- PMCID: PMC4833648
- DOI: 10.3174/ajnr.A4631
Computational Identification of Tumor Anatomic Location Associated with Survival in 2 Large Cohorts of Human Primary Glioblastomas
Abstract
Background and purpose: Tumor location has been shown to be a significant prognostic factor in patients with glioblastoma. The purpose of this study was to characterize glioblastoma lesions by identifying MR imaging voxel-based tumor location features that are associated with tumor molecular profiles, patient characteristics, and clinical outcomes.
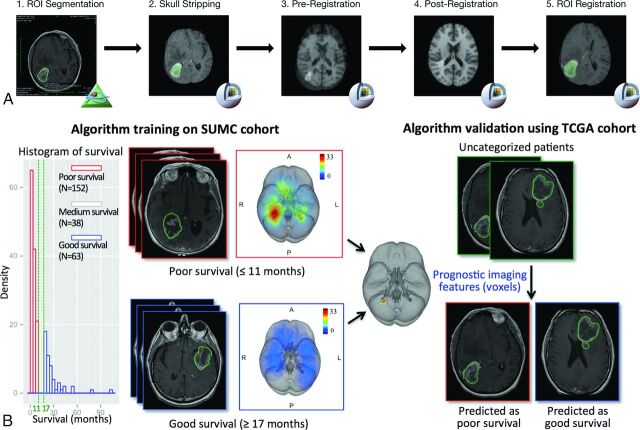
Materials and methods: Preoperative T1 anatomic MR images of 384 patients with glioblastomas were obtained from 2 independent cohorts (n = 253 from the Stanford University Medical Center for training and n = 131 from The Cancer Genome Atlas for validation). An automated computational image-analysis pipeline was developed to determine the anatomic locations of tumor in each patient. Voxel-based differences in tumor location between good (overall survival of >17 months) and poor (overall survival of <11 months) survival groups identified in the training cohort were used to classify patients in The Cancer Genome Atlas cohort into 2 brain-location groups, for which clinical features, messenger RNA expression, and copy number changes were compared to elucidate the biologic basis of tumors located in different brain regions.
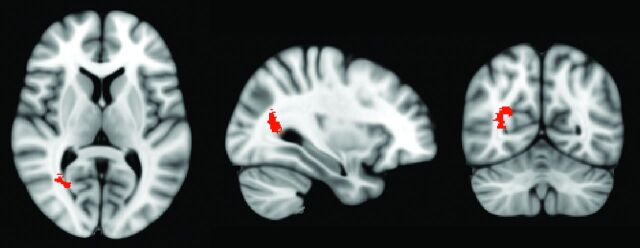
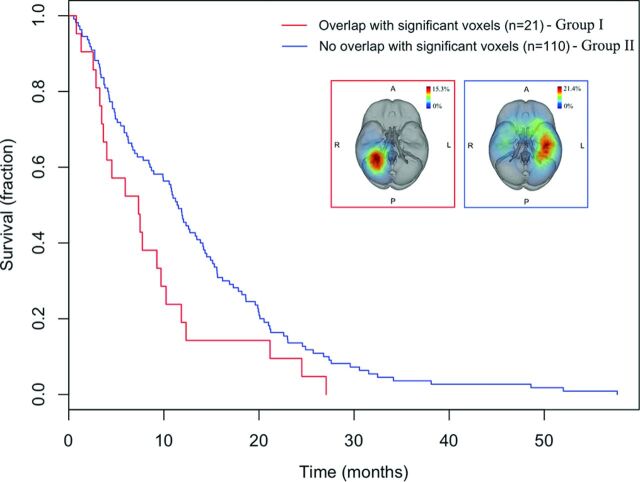
Results: Tumors in the right occipitotemporal periventricular white matter were significantly associated with poor survival in both training and test cohorts (both, log-rank P < .05) and had larger tumor volume compared with tumors in other locations. Tumors in the right periatrial location were associated with hypoxia pathway enrichment and PDGFRA amplification, making them potential targets for subgroup-specific therapies.
Conclusions: Voxel-based location in glioblastoma is associated with patient outcome and may have a potential role for guiding personalized treatment.
© 2016 by American Journal of Neuroradiology.
Figures
References
-
- Verhaak RG, Hoadley KA, Purdom E, et al. ; Cancer Genome Atlas Research Network. Integrated genomic analysis identifies clinically relevant subtypes of glioblastoma characterized by abnormalities in PDGFRA, IDH1, EGFR, and NF1. Cancer Cell 2010;17:98–110 10.1016/j.ccr.2009.12.020 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous