

Case Reports
doi: 10.1016/j.rmcr.2015.09.011.
eCollection 2015.
Sarcoidosis as unusual cause of massive pleural effusion
Affiliations
- PMID: 26744683
- PMCID: PMC4682006
- DOI: 10.1016/j.rmcr.2015.09.011
Item in Clipboard
Case Reports
Sarcoidosis as unusual cause of massive pleural effusion
Respir Med Case Rep.
.
Abstract
Sarcoidosis is a multisystem granulomatous disease of unknown etiology. Pleural involvement is relatively rare. Development of pleural effusion in sarcoidosis needs to be evaluated for other causes, especially tuberculosis in endemic countries. Sarcoid pleural effusion responds to systemic corticosteroids. We are presenting case of 42 year old male patient of sarcoidosis who developed massive pleural effusion while on treatment with steroids, which was attributed to disease per se. Sarcoidosis as a cause of massive pleural effusion has not been mentioned before in published literature.
Keywords: Effusion; Sarcoidosis; Thoracoscopy.
Figures

A: Chest X-ray in previous admission-showing Diffuse nodular shadows. B: CT-chest on previous admission – showing diffuse micronodules with prediliction for fissures and bronchovascular bundles.
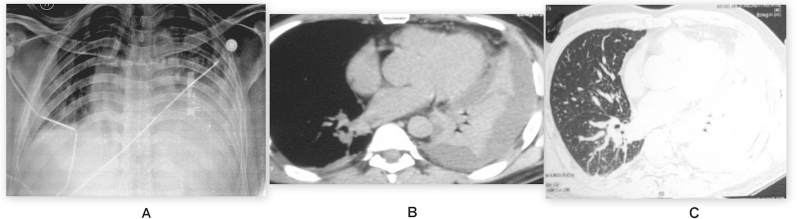
A: Chest X-ray on presentation-Homogenous opacity of left lower zone with blunt costophrenic angle. B: CT-chest Mediastinal window – showing Pleural effusion with atelectasis on left side. C: CT-chest Lung window.

A: Pleuroscopic view of Visceral pleura showing multiple nodular lesions. B: Pleuroscopic View of irregular and nodular diaphragmatic pleura.

A: Bronchoscopic Picture showing irregular and edematous bronchial mucosa (B6). B: Endobronchial Biopsy showing noncaseating epitheloid cell granulomas. C: Transbronchial lung biopsy showing ill formed epithelioid granulomas.
References
-
- Soskel N.T., Sharma O.P. Pleural involvement in sarcoidosis: case presentation and detailed review of the literature. Curr. Opin. Pulm. Med. 2000;6:455–468. - PubMed
-
- Huggins J.T., Doelken P., Sahn S.A. Pleural effusions in a series of 181 outpatients with sarcoidosis. Chest. 2006;129:1599–1604. - PubMed
-
- Gordonson J., Trachtenberg S., Sargent E.N. Superior vena cava obstruction due to sarcoidosis. Chest. 1973;63:292–293. - PubMed
-
- Poe R.H. Middle-lobe atelectasis. N. Y. State J. Med. 1978;78:2895–2897. - PubMed
-
- Heidecker J.T., Judson M.A. Pleural effusion caused by a trapped lung. South Med. J. 2003;96:510–511. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
