

Review
doi: 10.1097/GRF.0000000000000164.
Epidemiology of Uterine Fibroids: From Menarche to Menopause
Affiliations
- PMID: 26744813
- PMCID: PMC4733579
- DOI: 10.1097/GRF.0000000000000164
Item in Clipboard
Review
Epidemiology of Uterine Fibroids: From Menarche to Menopause
Clin Obstet Gynecol.
2016 Mar.
Abstract
Uterine leiomyomata (UL) have a substantial impact on women's health, but relatively few studies have identified opportunities for primary prevention of these neoplasms. Most established risk factors are not modifiable, including premenopausal age, African ancestry, age at menarche, and childbearing history. The main challenge in studying UL is that a large proportion of tumors are asymptomatic. Herein, we review the epidemiology of UL from published studies to date. We highlight the advantages of ultrasound screening studies and the ways in which their innovative methods have helped clarify the etiology of disease. We conclude with a discussion of promising new hypotheses.
Figures
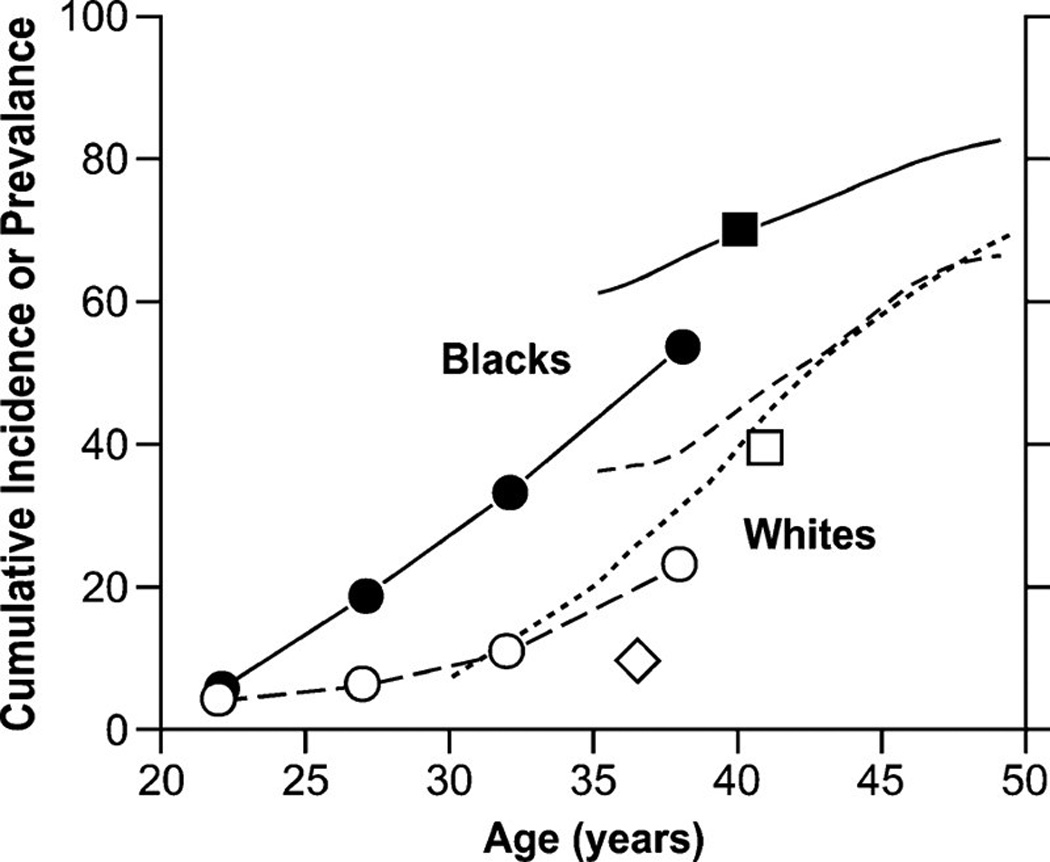
Age-specific cumulative incidence or prevalence estimates of uterine leiomyomata based on ultrasound-screening studies. The closed and open circles are prevalence data averaged over the age ranges shown for black and white women participating in Right from the Start [82], a community-based pregnancy study that screens for leiomyomata at ~7 weeks of gestation. The solid line and line of long dashes are cumulative incidence data from the UFS [14] a study of 35- to 49-year-old health plan members whose case status was based on either ultrasound screening for uterine leiomyomata (premenopausal women) or on prior diagnosis of uterine leiomyomata (postmenopausal women). The line of short dashes is cumulative incidence data from the low-exposed group of potentially dioxin-exposed women (Seveso, Italy) [9, 26, 87], 30- to 50-year-olds whose case status was based on either ultrasound screening for uterine leiomyomata (premenopausal women) or on prior diagnosis of uterine leiomyomata (postmenopausal women). The squares are average cumulative incidence data for samples of 33- to 46-year-old black and white participants in the Coronary Artery Risk Development in Young Adults study [25], a population-based study of cardiovascular disease. The diamond is the average prevalence of uterine leiomyomata for a group of 33- to 40-year-old representative Swedish women who had ultrasound screening for uterine leiomyomata [15].
References
-
- Merrill RM. Hysterectomy surveillance in the United States, 1997 through 2005. Med Sci Monit. 2008;14(1):CR24–CR31. - PubMed
-
- Becker ER. National trends and determinants of hospitalization costs and lengths-of-stay for uterine fibroids procedures. Journal of Health Care Finance. 2007;33(3):1–16. - PubMed
-
- Whiteman MK, et al. Inpatient hospitalization for gynecologic disorders in the United States. Am J Obstet Gynecol. 2010;202(6):541 e1–541 e6. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
