

Global Consensus Recommendations on Prevention and Management of Nutritional Rickets
- PMID: 26745253
- PMCID: PMC4880117
- DOI: 10.1210/jc.2015-2175
Global Consensus Recommendations on Prevention and Management of Nutritional Rickets
Abstract
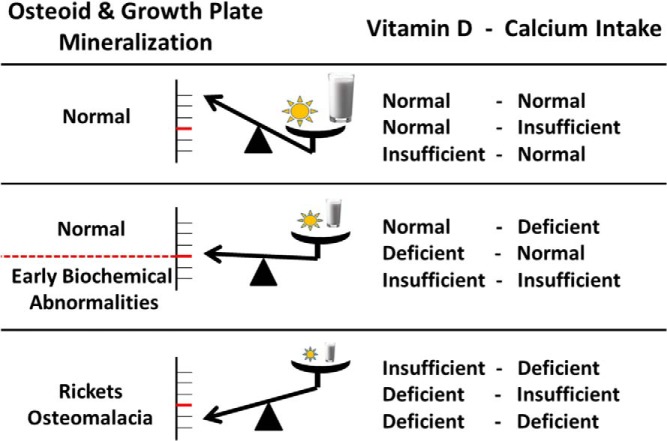
Background: Vitamin D and calcium deficiencies are common worldwide, causing nutritional rickets and osteomalacia, which have a major impact on health, growth, and development of infants, children, and adolescents; the consequences can be lethal or can last into adulthood. The goals of this evidence-based consensus document are to provide health care professionals with guidance for prevention, diagnosis, and management of nutritional rickets and to provide policy makers with a framework to work toward its eradication.
Evidence: A systematic literature search examining the definition, diagnosis, treatment, and prevention of nutritional rickets in children was conducted. Evidence-based recommendations were developed using the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) system that describe the strength of the recommendation and the quality of supporting evidence.
Process: Thirty-three nominated experts in pediatric endocrinology, pediatrics, nutrition, epidemiology, public health, and health economics evaluated the evidence on specific questions within five working groups. The consensus group, representing 11 international scientific organizations, participated in a multiday conference in May 2014 to reach a global evidence-based consensus.
Results: This consensus document defines nutritional rickets and its diagnostic criteria and describes the clinical management of rickets and osteomalacia. Risk factors, particularly in mothers and infants, are ranked, and specific prevention recommendations including food fortification and supplementation are offered for both the clinical and public health contexts.
Conclusion: Rickets, osteomalacia, and vitamin D and calcium deficiencies are preventable global public health problems in infants, children, and adolescents. Implementation of international rickets prevention programs, including supplementation and food fortification, is urgently required.
Figures
Comment in
-
Response to the letter by Sugiyama and Oda.J Clin Endocrinol Metab. 2016 Oct;101(10):L97-L98. doi: 10.1210/jc.2016-3059. J Clin Endocrinol Metab. 2016. PMID: 27702314 No abstract available.
-
Letter to the Editor: Vitamin D Deficiency and Fractures in Children: A Mechanistic Point of View.J Clin Endocrinol Metab. 2016 Oct;101(10):L95-L96. doi: 10.1210/jc.2016-2651. J Clin Endocrinol Metab. 2016. PMID: 27702315 No abstract available.
References
-
- Munns CF, Simm PJ, Rodda CP, et al. Incidence of vitamin D deficiency rickets among Australian children: an Australian Paediatric Surveillance Unit study. Med J Aust. 2012;196(7):466–468. - PubMed
-
- Beck-Nielsen SS, Jensen TK, Gram J, Brixen K, Brock-Jacobsen B. Nutritional rickets in Denmark: a retrospective review of children's medical records from 1985 to 2005. Eur J Pediatr. 2009;168(8):941–949. - PubMed
-
- Thacher TD, Fischer PR, Pettifor JM, et al. A comparison of calcium, vitamin D, or both for nutritional rickets in Nigerian children. N Engl J Med. 1999;341(8):563–568. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
