

Atrial Fibrillation Begets Heart Failure and Vice Versa: Temporal Associations and Differences in Preserved Versus Reduced Ejection Fraction
- PMID: 26746177
- PMCID: PMC4738087
- DOI: 10.1161/CIRCULATIONAHA.115.018614
Atrial Fibrillation Begets Heart Failure and Vice Versa: Temporal Associations and Differences in Preserved Versus Reduced Ejection Fraction
Abstract
Background: Atrial fibrillation (AF) and heart failure (HF) frequently coexist and together confer an adverse prognosis. The association of AF with HF subtypes has not been well described. We sought to examine differences in the temporal association of AF and HF with preserved versus reduced ejection fraction.
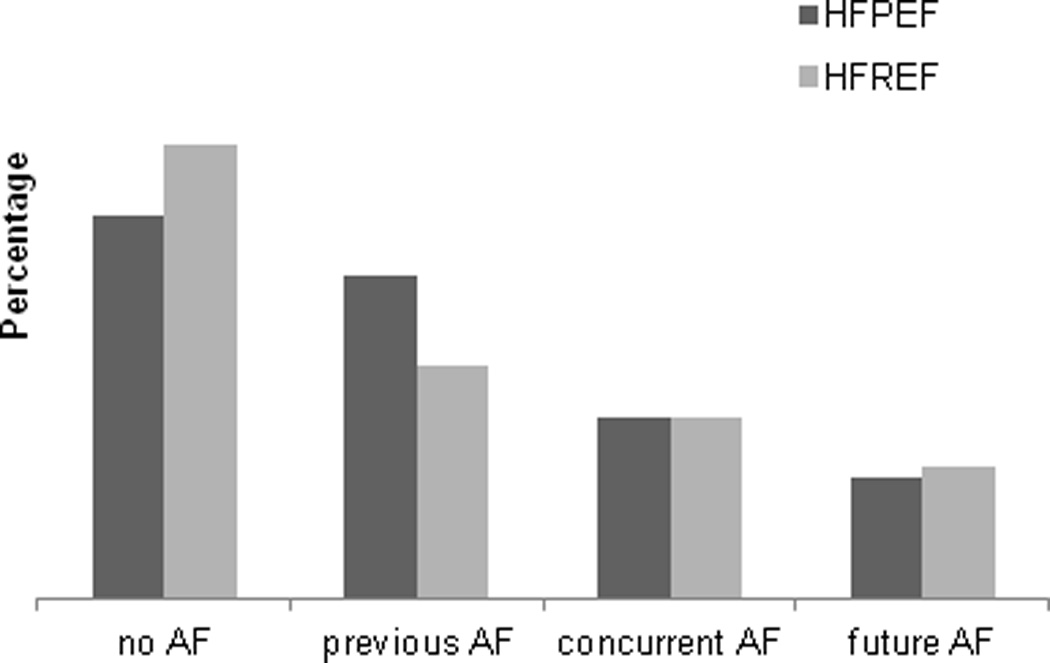
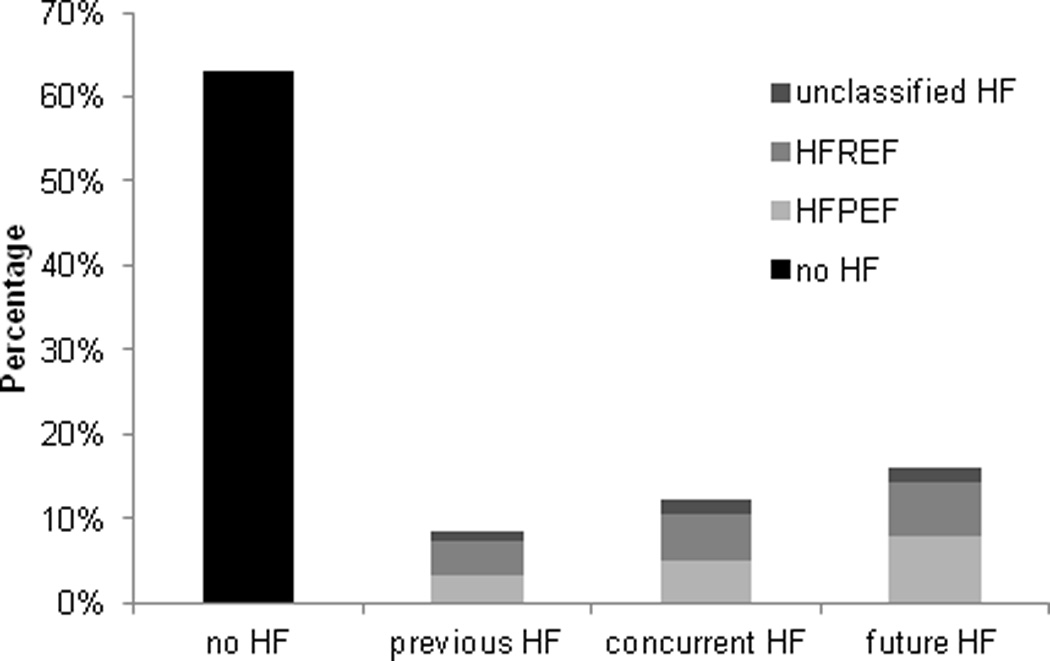
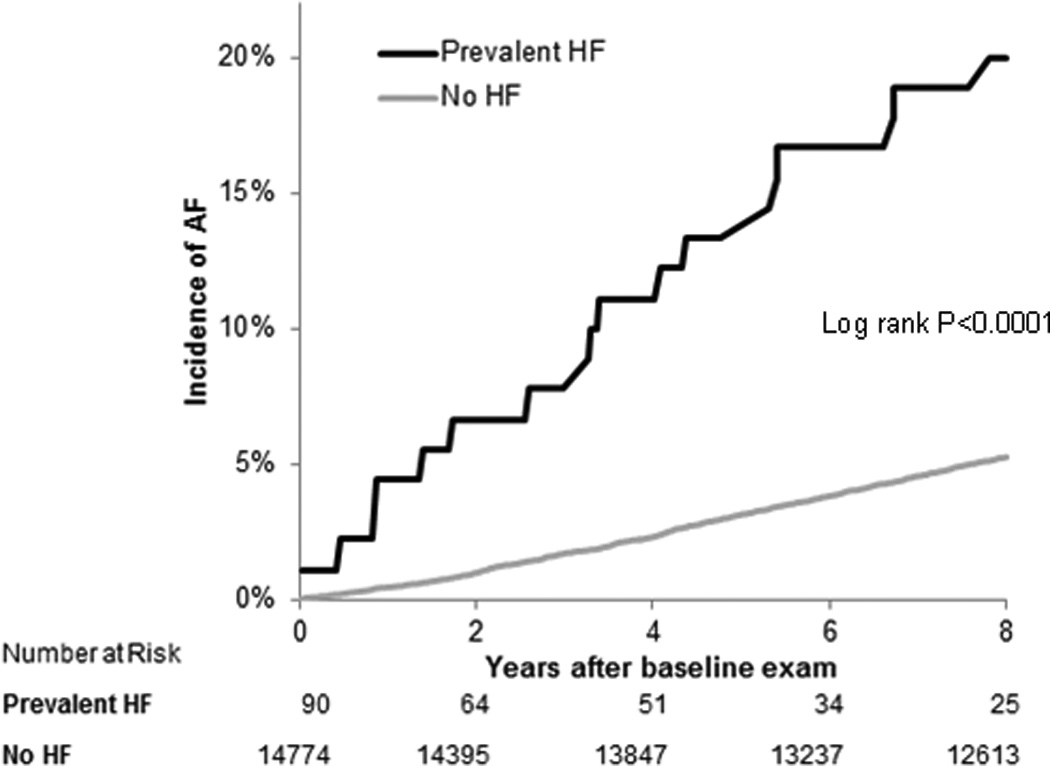
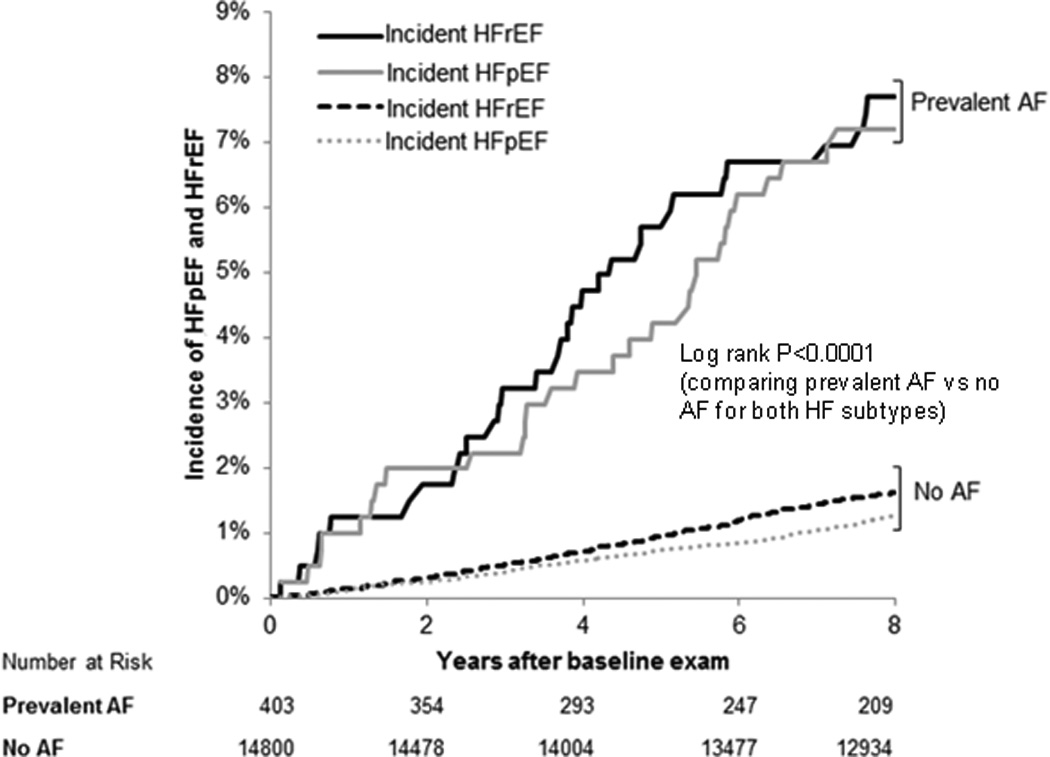
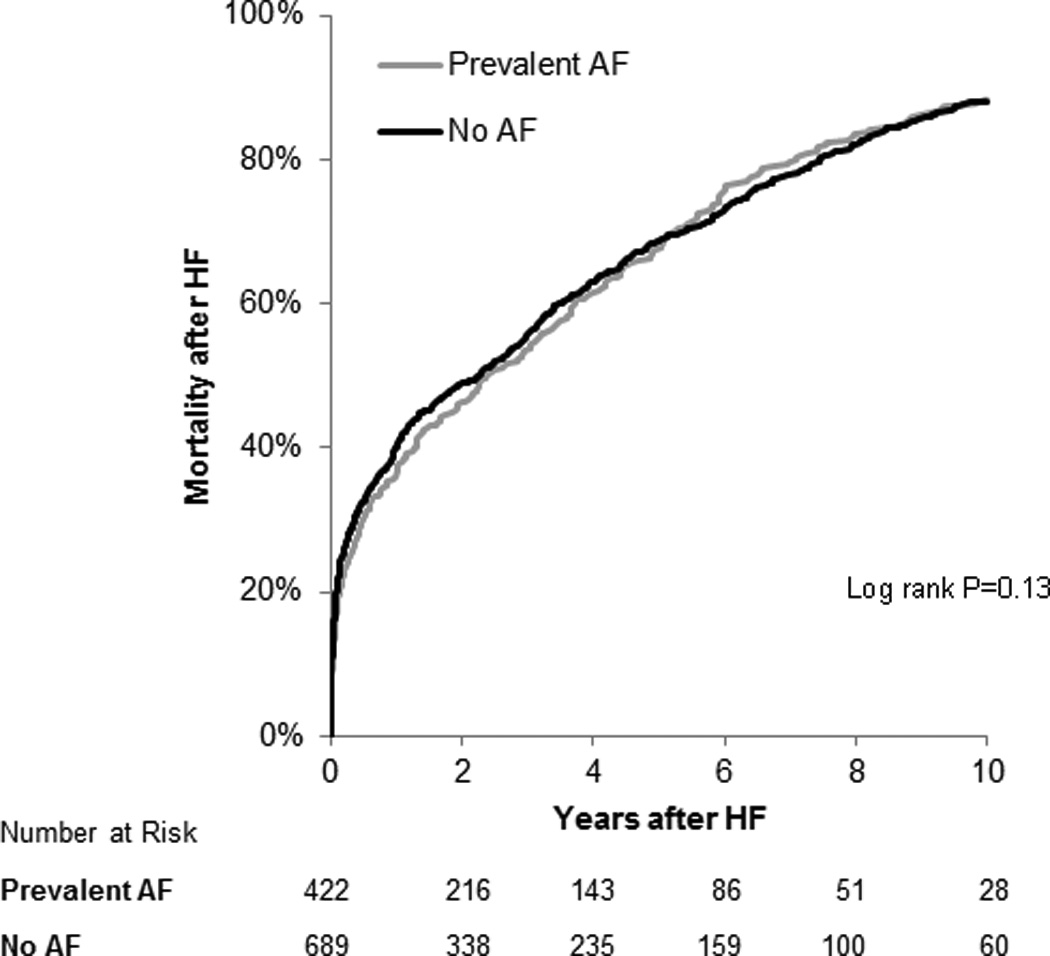
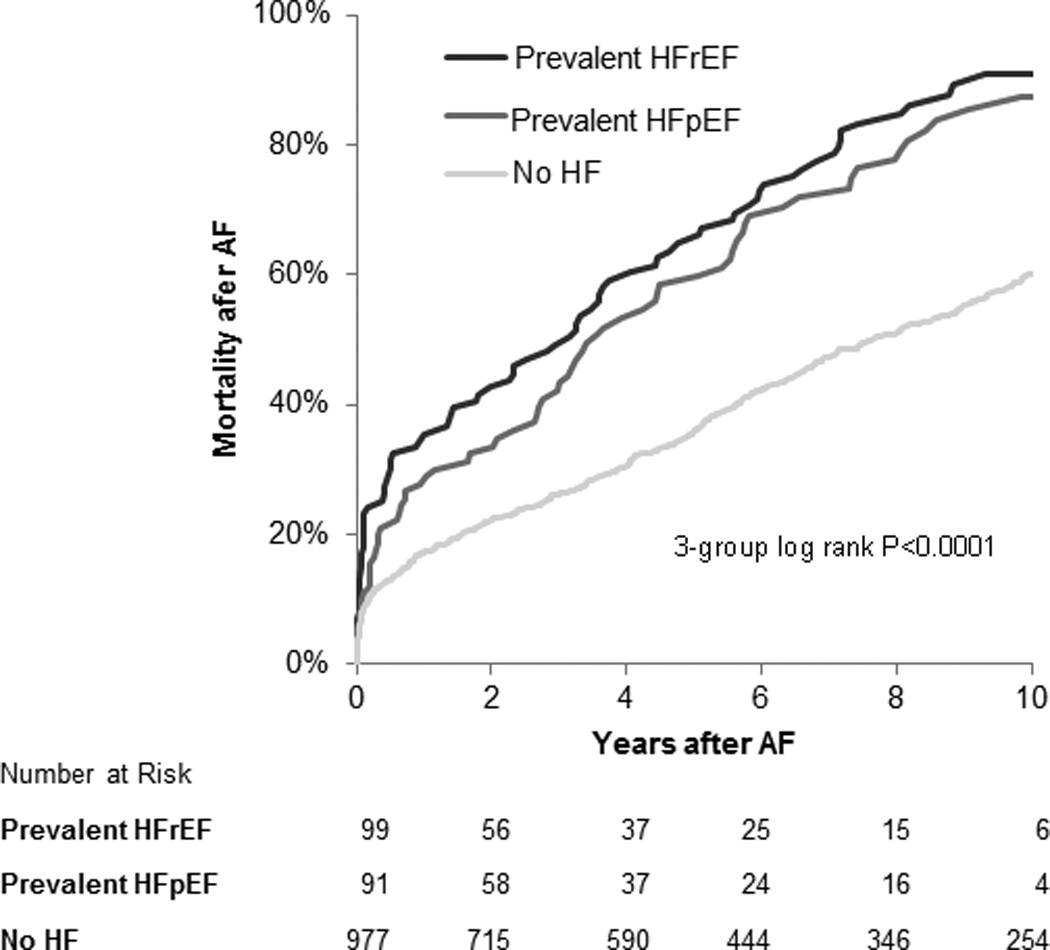
Methods and results: We studied Framingham Heart Study participants with new-onset AF or HF between 1980 and 2012. Among 1737 individuals with new AF (mean age, 75±12 years; 48% women), more than one third (37%) had HF. Conversely, among 1166 individuals with new HF (mean age, 79±11 years; 53% women), more than half (57%) had AF. Prevalent AF was more strongly associated with incident HF with preserved ejection fraction (multivariable-adjusted hazard ratio [HR], 2.34; 95% confidence interval [CI], 1.48-3.70; no AF as referent) versus HF with reduced ejection fraction (HR, 1.32; 95% CI, 0.83-2.10), with a trend toward difference between HF subtypes (P for difference=0.06). Prevalent HF was associated with incident AF (HR, 2.18; 95% CI, 1.26-3.76; no HF as referent). The presence of both AF and HF portended greater mortality risk compared with neither condition, particularly among individuals with new HF with reduced ejection fraction and prevalent AF (HR, 2.72; 95% CI, 2.12-3.48) compared with new HF with preserved ejection fraction and prevalent AF (HR, 1.83; 95% CI, 1.41-2.37; P for difference=0.02).
Conclusions: AF occurs in more than half of individuals with HF, and HF occurs in more than one third of individuals with AF. AF precedes and follows HF with both preserved and reduced ejection fraction, with some differences in temporal association and prognosis. Future studies focused on underlying mechanisms of these dual conditions are warranted.
Keywords: atrial fibrillation; epidemiology; heart failure; mortality; ventricular function, left.
© 2016 American Heart Association, Inc.
Figures
Comment in
-
Letter by Providencia and Lambiase Regarding Article, "Atrial Fibrillation Begets Heart Failure and Vice Versa: Temporal Associations and Differences in Preserved Versus Reduced Ejection Fraction".Circulation. 2016 Jun 7;133(23):e691. doi: 10.1161/CIRCULATIONAHA.116.021563. Circulation. 2016. PMID: 27267540 No abstract available.
-
Response to Letter Regarding Article, "Atrial Fibrillation Begets Heart Failure and Vice Versa: Temporal Associations and Differences in Preserved Versus Reduced Ejection Fraction".Circulation. 2016 Jun 7;133(23):e692-3. doi: 10.1161/CIRCULATIONAHA.116.022835. Circulation. 2016. PMID: 27267541 Free PMC article. No abstract available.
References
-
- Braunwald E. Shattuck lecture--cardiovascular medicine at the turn of the millennium: triumphs, concerns, and opportunities. N Engl J Med. 1997;337:1360–1369. - PubMed
-
- Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cushman M, de Ferranti S, Després J, Fullerton HJ, Howard VJ, Huffman MD, Judd SE, Kissela BM, Lackland DT, Lichtman JH, Lisabeth LD, Liu S, Mackey RH, Matchar DB, McGuire DK, Mohler ER, Moy CS, Muntner P, Mussolino ME, Nasir K, Neumar RW, Nichol G, Palaniappan L, Pandey DK, Reeves MJ, Rodriguez CJ, Sorlie PD, Stein J, Towfighi A, Turan TN, Virani SS, Willey JZ, Woo D, Yeh RW, Turner MB. American Heart Association Statistics Committee, Subcommittee SS. Heart disease and stroke statistics-2015 update: a report from the American Heart Association. Circulation. 2015;131:e29–e322. - PubMed
-
- Colilla S, Crow A, Petkun W, Singer DE, Simon T, Liu X. Estimates of current and future incidence and prevalence of atrial fibrillation in the U.S. adult population. Am J Cardiol. 2013;112:1142–1147. - PubMed
-
- Ho KK, Anderson KM, Kannel WB, Grossman W, Levy D. Survival after the onset of congestive heart failure in Framingham Heart Study subjects. Circulation. 1993;88:107–115. - PubMed
Publication types
MeSH terms
Grants and funding
- N01-HC-25195/HC/NHLBI NIH HHS/United States
- 2R01HL092577/HL/NHLBI NIH HHS/United States
- HHSN268201500001C/HL/NHLBI NIH HHS/United States
- R01 HL092577/HL/NHLBI NIH HHS/United States
- 1R01HL128914/HL/NHLBI NIH HHS/United States
- N01 HC025195/HC/NHLBI NIH HHS/United States
- K23-HL116780/HL/NHLBI NIH HHS/United States
- 3R01HL092577-06S1/HL/NHLBI NIH HHS/United States
- R01 HL128914/HL/NHLBI NIH HHS/United States
- N01 HC025195/HL/NHLBI NIH HHS/United States
- HHSN268201500001I/HL/NHLBI NIH HHS/United States
- K23 HL116780/HL/NHLBI NIH HHS/United States
- 2014105/DDCF/Doris Duke Charitable Foundation/United States
- K23 HL114724/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
