

The History and Future of Treatment of Hypothyroidism
- PMID: 26747302
- PMCID: PMC4980994
- DOI: 10.7326/M15-1799
The History and Future of Treatment of Hypothyroidism
Erratum in
-
Correction: History and Future of Treatment of Hypothyroidism.Ann Intern Med. 2016 Mar 1;164(5):376. doi: 10.7326/L16-0022. Ann Intern Med. 2016. PMID: 26926699
Abstract
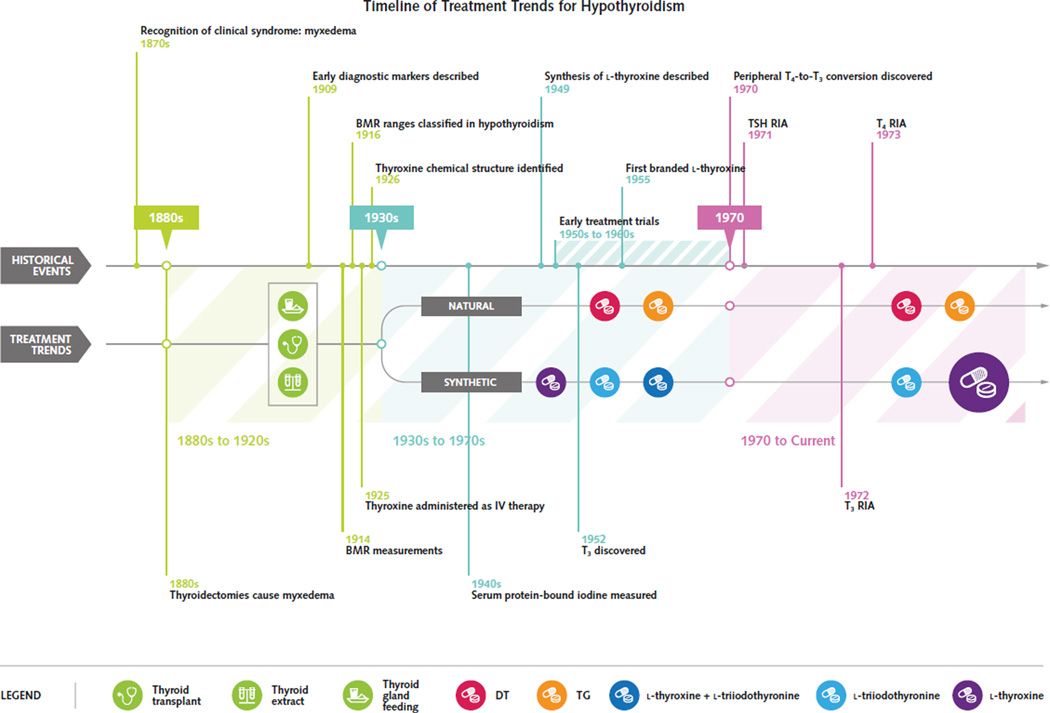
Thyroid hormone replacement has been used for more than a century to treat hypothyroidism. Natural thyroid preparations (thyroid extract, desiccated thyroid, or thyroglobulin), which contain both thyroxine (T4) and triiodothyronine (T3), were the first pharmacologic treatments available and dominated the market for the better part of the 20th century. Dosages were adjusted to resolve symptoms and to normalize the basal metabolic rate and/or serum protein-bound iodine level, but thyrotoxic adverse effects were not uncommon. Two major developments in the 1970s led to a transition in clinical practice: 1) The development of the serum thyroid-stimulating hormone (TSH) radioimmunoassay led to the discovery that many patients were overtreated, resulting in a dramatic reduction in thyroid hormone replacement dosage, and 2) the identification of peripheral deiodinase-mediated T4-to-T3 conversion provided a physiologic means to justify l-thyroxine monotherapy, obviating concerns about inconsistencies with desiccated thyroid. Thereafter, l-thyroxine monotherapy at doses to normalize the serum TSH became the standard of care. Since then, a subgroup of thyroid hormone-treated patients with residual symptoms of hypothyroidism despite normalization of the serum TSH has been identified. This has brought into question the inability of l-thyroxine monotherapy to universally normalize serum T3 levels. New research suggests mechanisms for the inadequacies of l-thyroxine monotherapy and highlights the possible role for personalized medicine based on deiodinase polymorphisms. Understanding the historical events that affected clinical practice trends provides invaluable insight into formulation of an approach to help all patients achieve clinical and biochemical euthyroidism.
Conflict of interest statement
Figures
References
-
- Jonklaas J, Bianco AC, Bauer AJ, Burman KD, Cappola AR, Celi FS, et al. American Thyroid Association Task Force on Thyroid Hormone Replacement. Guidelines for the treatment of hypothyroidism: prepared by the American Thyroid Association Task Force on Thyroid Hormone Replacement. Thyroid. 2014;24:1670–1751. [PMID: 25266247] - PMC - PubMed
-
- Saravanan P, Chau WF, Roberts N, Vedhara K, Greenwood R, Dayan CM. Psychological well-being in patients on ‘adequate’ doses of l-thyroxine: results of a large, controlled community-based questionnaire study. Clin Endocrinol (Oxf) 2002;57:577–585. [PMID: 12390330] - PubMed
Web-Only References
-
- Means JH. The Thyroid and Its Diseases. 2nd. Philadelphia: JB Lippincott; 1948. Myxedema; pp. 241–273.
-
- Soffer LJ. Diseases of the Endocrine Glands. 2nd. Philadelphia: Lea & Febiger; 1956. Hypothyroidism: cretinism, juvenile and adult myx-edema (Gulls’ disease) pp. 829–868.
-
- Williams RH, Bakke JL. General consideration of the treatment of thyroid disease. In: Williams RH, editor. Textbook of Endocrinology. 3rd. Philadelphia: WB Saunders; 1962. pp. 133–135.
-
- Pittman JA. Diagnosis and Treatment of Thyroid Diseases. Philadelphia: FA Davis; 1963. Hypothyroidism; pp. 56–78.
-
- Hoffenberg R. Primary hypothyroidism. In: Ingbar SH, Braverman LE, editors. Werner’s The Thyroid: A Fundamental and Clinical Text. 5th. Philadelphia: JB Lippincott; 1986. pp. 1255–1265.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical