

Cancer Therapy-Related Cardiac Dysfunction and Heart Failure: Part 1: Definitions, Pathophysiology, Risk Factors, and Imaging
- PMID: 26747861
- PMCID: PMC4709035
- DOI: 10.1161/CIRCHEARTFAILURE.115.002661
Cancer Therapy-Related Cardiac Dysfunction and Heart Failure: Part 1: Definitions, Pathophysiology, Risk Factors, and Imaging
Abstract
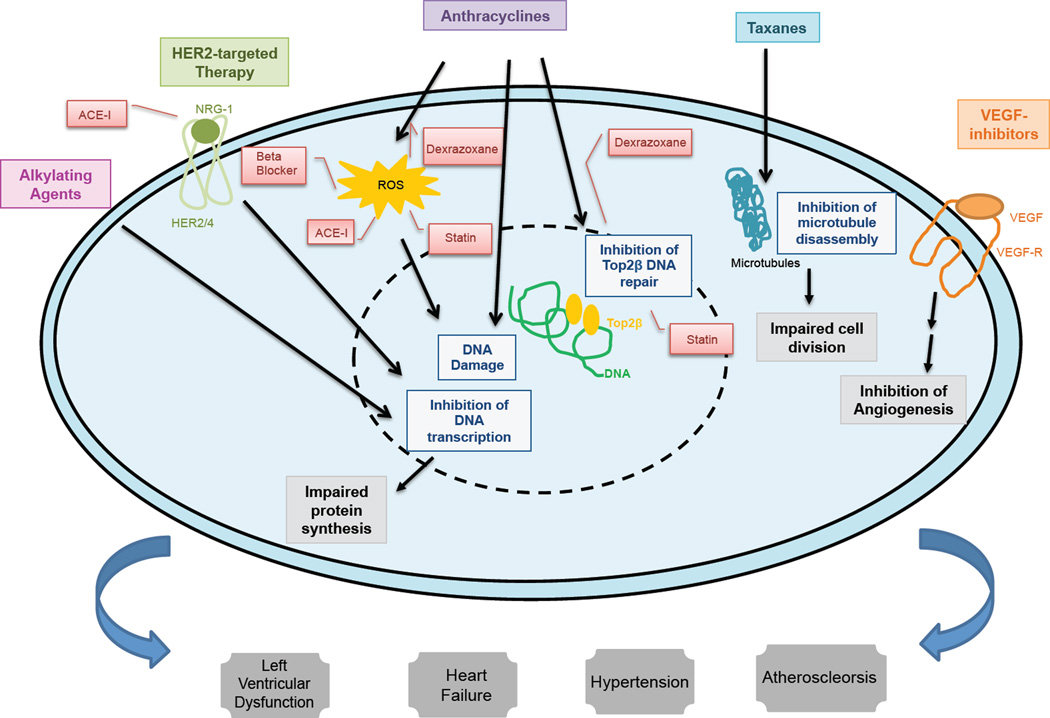
Advances in cancer therapy have resulted in significant improvement in long-term survival for many types of cancer but have also resulted in untoward side effects associated with treatment. One such complication that has become increasingly recognized is the development of cardiomyopathy and heart failure. Whether a previously healthy person from a cardiovascular perspective develops cancer therapy-related cardiac dysfunction or a high-risk cardiovascular patient requires cancer therapy, the team of oncologists and cardiologists must be better equipped with an evidence-based approach to care for these patients across the spectrum. Although the toxicities associated with various cancer therapies are well recognized, limitations to our understanding of the appropriate course of action remain. In this first of a 2-part review, we discuss the epidemiologic, pathophysiologic, risk factors, and imaging aspects of cancer therapy-related cardiac dysfunction and heart failure. In a subsequent second part, we discuss the prevention and treatment aspects, concluding with a section on evidence gap and future directions. We focus on adult patients in all stages of cancer therapy from pretreatment surveillance, to ongoing therapy, and long-term follow-up.
Keywords: anthracyclines; cardiomyopathies; cardiotoxicity; chemotherapy; heart failure; trastuzumab; ventricular dysfunction, left.
© 2016 American Heart Association, Inc.
Conflict of interest statement
Figures
References
-
- Carver JR, Shapiro CL, Ng A, Jacobs L, Schwartz C, Virgo KS, Hagerty KL, Somerfield MR, Vaughn DJ. American Society of Clinical Oncology clinical evidence review on the ongoing care of adult cancer survivors: cardiac and pulmonary late effects. J Clin Oncol. 2007;25:3991–4008. - PubMed
-
- Silber JH, Cnaan A, Clark BJ, Paridon SM, Chin AJ, Rychik J, Hogarty AN, Cohen MI, Barber G, Rutkowski M, Kimball TR, Delaat C, Steinherz LJ, Zhao H. Enalapril to prevent cardiac function decline in long-term survivors of pediatric cancer exposed to anthracyclines. J Clin Oncol. 2004;22:820–828. - PubMed
-
- Rowinsky EKMW, Guarnieri T, Fisherman JS, Christian MC, Donehower RC. Cardiac disturbances during the administration of taxol. J Clin Oncol. 1991;9:1704–1712. - PubMed
-
- Sorrentino MFKJ, Eoderaro AE, Truesdell AG. 5-Fluorouracil induced cardiotoxicity: review of the literature. Cardiology Journal. 2012;19:453–458. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
